Volume 32, Issue 1: Paper 1
The Impact of Afghan Opium Cultivation on the American Opioid Epidemic
Zachary Cheek, University of Nebraska at Lincoln
Aside from the COVID-19 pandemic, the American opioid epidemic is recognized as the most dire public health crisis in U.S. history. A problem long before the pandemic, it is certainly expected to be a problem after.[1] Projections have placed the economic costs of the epidemic as well over a trillion dollars,[2] and increasing by even more each year.[3] While the epidemic has mostly affected white urban and suburban citizens,[4] recent evidence has shown detrimental effects among black, Native American, and Hispanic communities as well.[5] The crisis has largely contributed to recent declines in Americans’ life expectancies[6] as well as labor force participation.[7] Thus, when potentially considering the nature and economics of opioids, the question begs itself for the sake of Americans’ lives. And the first step towards solving any problem in policy is truly understanding it.
Opioids, whether legal (prescribed) or illegal (smuggled medications, heroin, etc.) follow the characteristics of a market system.[8] Vast literature has proven that, for a long time, lower prices have led to higher amounts demanded (in other words, that the law of demand applies) (see Literature Review); that ease of access and similarity in effect allow for competing substitutes between types of opioid[9]; and finally, that outside factors, such as government disruptions[10] or cheaper production costs, will have direct (though not necessarily intended) ramifications for “consumers.” Furthermore, addicts need not be hardened drug dealers; many were and are everyday people with legitimate medical needs, who found the potent effects of opiates impossible to quit.
This paper focuses on a key aspect of production costs. Essentially, in the same way that an increase in Brazilian sugar, for example, would presumably lead to lower candy prices and more cavities among small children, it is argued here that an increase in opium production overseas has led to lower opium derivative prices and higher overdose death rates across the already-interconnected world market. All heroin in the United States for instance is foreign-sourced,[11] incentivizing illicit diversion through lower prices; cheaper opium overall incentivizes diversion from the legal prescription market to the illicit one.[12] It so follows that the focus of this research is the world’s largest opium producer: Afghanistan, a nation whose internal production of poppy (Papaver Somniferum L.) alone over the past several decades has averaged more than three-quarters of world opium output.
Examining the years 1999 to 2018 (the only years for which there are readily available public health data), this study estimates the relationship between Afghan opium growth, indicators of prescription opioid/heroin prices, and population-adjusted overdose death rates in the United States. While the study relates to the prodigious empirical literature regarding consumer responsiveness to changes in opioid prices, it builds upon it by attempting to account for the role of Afghan opium in depressing these prices. In doing so, it also helps shed light on an under-examined aspect of one of the greatest public health issues in American history.
II. The American Opioid Epidemic
The pervasiveness of physical pain, interfering with work and daily life for many, has been on the rise since at least 1997,[13] and opioids are a key way in which these issues have been addressed. In 1986, Drs. Russell Portenoy and Kathleen Foley published a now infamous study examining 38 patients’ individual pain needs relative to what opioids could then treat. They concluded that in certain low-risk populations, opioids were an effective and nonaddictive means of treating chronic noncancer pain,[14] and opioid prescribing rates exploded from there.[15]. The drugs became so prevalent in prescription pain treatments that providers within the industry unwilling to follow suit were even described as “careless, naive, and unsympathetic.”[16]
Several pharmaceutical companies helped medical advocacy groups, healthcare providers, and state medical boards argue to federal regulators that addiction was a minimal and exaggerated threat to patients.[17] The pressure on doctors to commit medical malpractice in overprescribing was quite real, and perhaps even lasts to this day.[18]
The implications of such high accessibility were wide-reaching. As reported by Inciardi et al.,[19] opioids were accessible from domestic healthcare providers (including ones selected by patients for this express purpose), trips overseas, and black markets, and even through theft among friends and relatives. Lobbying by companies had reached a boiling point by 1995, when Purdue Pharmaceuticals (a corporation involved in many recent lawsuits) was approved by the Food and Drug Administration to market the powerful opioid formulation OxyContin.[20]
While OxyContin’s pill form releases the painkiller oxycodone gradually over twelve hours, when it is crushed, dissolved, or injected, the drug releases all at once, making abuse incredibly easy.[21] While this paper will discuss the price elasticity of opioids (the responsiveness of changes in price to changes in quantity demanded) later on, it is worth noting that a regulatory and commercial environment was meticulously created through these many efforts in which consumers, addicts, and patients were empowered to respond to price changes in the first place.[22]
In 2010, a crush-resistant, controlled-release drug formulation began to be marketed instead as a way to lower abuse risk. However, this development instead had an extremely adverse effect on public health; while OxyContin use did indeed decline,[23] the new heroin crisis began almost immediately after reformulation. Following a steady rise in U.S. heroin deaths per capita that drove the opioid crisis’ increase until 2013, and only recently began leveling off,[24] the sound consensus within the research community is that OxyContin’s reformulation significantly contributed to, if not caused, this great increase in heroin overdose deaths.[25]
Medically, as reported by Comer et al.,[26] the effect of heroin on the brain is indistinguishable from that of oxycodone or hydrocodone, and reliance on prescription opioids has been proven to increase the risk of reliance on heroin by a damning four thousand percent.[27] Past analyses have further proven that a majority of post-1990 heroin users began opioid abuse through prescriptions before switching.[28] In addition, while only a fraction of opioid abusers end up addicted to heroin, the proportion is large enough that, abstracted for the entire U.S. addict population, the burden on societal public health is undeniably concerning.[29]
The Council on Foreign Relations points out that:
[h]eroin for decades was the most commonly used illegal opioid, as the supply of the drug in the United States soared and its average retail-level price dropped by the mid-2010s to roughly one-third of what it was in the early 1980s.[30]
To make matters worse, the frequent use of unsanitary needles by heroin users also contributes to HIV, AIDS, and Hepatitis outbreaks nationwide.[31]
Around 2013, dealers began lacing drugs with fentanyl, a chemically-derived drug that does not use opium. The switch for dealers from heroin to fentanyl was driven by the latter’s much lower cost and potency,[32] allowing even higher profit margins. Fentanyl is legal in some cases; prevalent as an ultra-potent painkiller, it is often medically associated with terminally-ill patients.[33] Carfentanyl, a synthetic derivative a hundred times more potent (and often used as a tranquilizer for elephants), is so dangerous that it even poses risk to law enforcement officials at crime scenes.[34]
It is worth mentioning that dealers’ newfound affinity for fentanyl does not mean that the heroin epidemic has “died down.” Fentanyl simply grew more quickly. Indeed, as recently as 2017, the DEA[35] reported great alarm among local law enforcement officials towards heroin specifically.[36]
Most fentanyl smuggled into the United States originates in China through mail and legal ports of entry.[37] While the global fentanyl exchange is becoming increasingly diverse, now including India in addition to Mexico,[38] China has suffered massive drug policy inefficiencies, and has only recently begun to combat its fentanyl markets internally.[39] Unlike prescription fentanyl iterations (Actiq, Fentora, etc.), illicit fentanyl lacks checks on quality, hygiene, and purity, further increasing risk in consumption.[40] Furthermore, fentanyl overdoses are not shown in typical toxicology reports,[41] and necessitate separate, more specific tests. However, these tests are not always available in every American community, leading to uncertainty surrounding cause of death; consequently, up to twenty percent of coroners are not reliably able to determine the drug of causality in overdose deaths.[42]
Figure 1. The Three Waves of Opioid Overdose Deaths (Log), 1999 – 2018
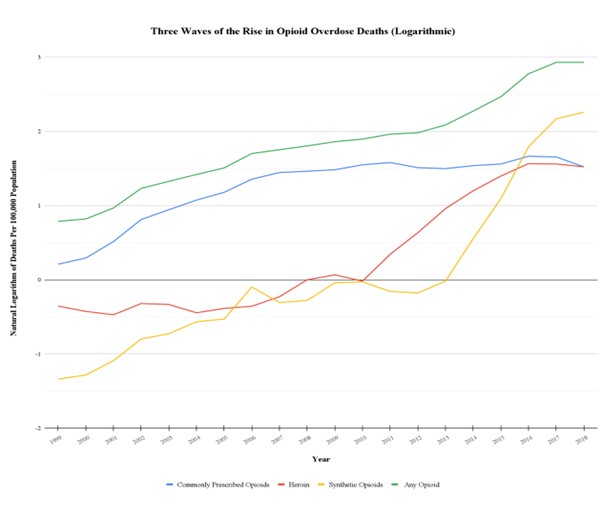
Source: Centers for Disease Control and Prevention[43]
As Figure 1 details above, the Centers for Disease Control and Prevention[44] estimate there to be three “waves” in the ongoing opioid crisis: prescription opioid-driven death increases from the 1990s (likely ca. 1995 due to the licensing of OxyContin) to 2009; heroin-driven death increases from 2010 to 2013; and synthetic opioid (namely fentanyl)-driven death increases from 2013 onward.[45] As shown, it was around 2009 and 2010 that heroin abuse and deaths became the key nonsynthetic driver of the increase in opioid deaths.
Major policy responses to the epidemic have included education for healthcare professionals and prosecuting smugglers domestically,[46] as well as making available the anti-overdose drug naloxone[47] and contributing to anti-drug operations conducted by governments overseas.[48] The future of the epidemic remains vague, as data describing the harm brought about during the COVID-19 pandemic have only recently become available.[49]
III. Afghan Opium Cultivation
Afghanistan was not always the world’s top opium supplier. However, over the course of the past four decades, Afghan opium cultivation has perniciously grown to its current point of domination in the global market.[50]
The epicenter of global production shifted there from Burma in the 1990s, growing from 51,000 poppy hectares cultivated in 1991 to 82,000 in 1999[51]. In 2006, 52% of Afghan gross domestic product was directly or indirectly derived from the illegal opium trade.[52]
The Afghan opium trade is “convergent,” meaning that one raw material (poppy) becomes one or a small number of end products (such as heroin).[53] Heroin is derived from opium through set-in-stone extraction, precipitation, purification, acetylation, and conversion steps. Furthermore, the number of morphine labs within Afghanistan itself are growing, thereby greatly reducing the weight of transported drugs and more easily enabling Asian, European, and Middle Eastern smuggling operations.[54]
The opium trade has fueled political instability, and instability in turn has fostered a more conducive political and economic environment in which to grow poppy. For many farmers, opium is the most water-efficient and profitable crop to grow.[55] So central is poppy to Afghan society nowadays that even innovations such as solar power have begun to be integrated into the production of opium.[56] Accordingly, domestic and international counter-narcotics campaigns have faltered largely out of an inability to provide families with viable long-term income alternatives.[57]
For most of this time, domestic counter-narcotics programs existed for nominal purposes at best. Corruption, rampant through rural Afghanistan, rendered government control over the market impotent,[58] with the notable exception of 2000-2001.[59] It was reported by the UNODC in 2009 that while nearly ninety percent of the world’s opium came from Afghanistan, less than two percent was seized there.[60]
As the Soviets retreated and the war ended, the drug-related conflict transitioned from political to economic.[61] The Taliban began to utilize opium as their main revenue arm, helping fund their armaments and human rights abuses in spite of international sanctions.[62] Regional instability in the decades following the Soviet-Afghan War has thereby led to substantial geographic concentration of poppy in the West and South of the country, where insurgencies have been most strong.[63]
After the Taliban came to power in 1997, several attempts at banning opium were unsuccessful until 2000. Attempting to gain international recognition of a Taliban government, as well as the rule of supreme leader Mullah Omar, the Taliban enforced their 2000 opium ban in one of the most successful anti-drug operations in history. Production fell over 90% from 2000 to 2001.[64] (This significant event will be examined later on in this study.)
Opium eradication measures in Afghanistan have not led to less poppy produced over time. Rather, it has resulted in greater poverty, government insecurity/insubordination, and even greater amounts produced as preemptive measures against eradication.[65]
Opium is now part of Afghan life. In 2003 and 2004, Afghan farmers reported high opium demand as one of the main reasons for which they grow opium.[66] Opium has even been reported to be the largest source of individual income in the entire nation.[67]
Congress has appropriated tens of millions of dollars in recent years to counternarcotics programs in the country.[68] Much of this has gone towards equipment and training for Afghan law enforcement, who in 2020 conducted over a hundred separate drug seizures.[69] Afghan opium production indeed has, in spite of domestic and international efforts, reached record-high levels, and now effectively dominates opium production in the world. See Figure 2 for a depiction of country-by-country production levels, as well as Table A for a chronology of Afghan opium. The former demonstrates Afghan dominance of global opium production, while the latter provides context from which this study can better provide chronologically-pertinent analysis.
Figure 2. Global Potential Production of Opium (Metric Tons), 1997 – 2018[70]
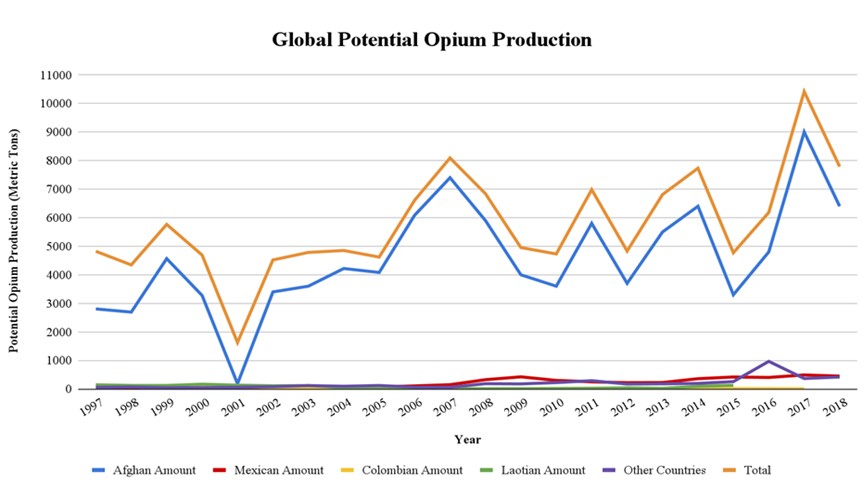
Source: United Nations Office on Drugs and Crime[71]
Table A. Timeline of the Political Economy of Afghan Opium Production, 1992 – Present
| Period | Description |
|---|---|
| 1992-1996 | Political order disintegrates and all factions in Afghan civil war engage in drug economy. Afghanistan becomes world’s largest producer of illicit opium. |
| 1996-2000 | Taliban regime gradually establishes control; cultivation continues to flourish. |
| 2000-2001 | Widely enforced Taliban ban on cultivation leads to a drastic drop in cultivation during the 2000-2001 growing season. |
| 2002-2008 | Overthrow of Taliban regime and rising global opium prices leads to resurgence of cultivation; expansion of cultivation to northern and central regions as well as significant growth in south; many officials in new regime linked to drug economy. |
| 2008-2011 | Counter-narcotics initiatives and declining global prices lead to overall declines in opium production, though bans were inconsistently enforced. |
| 2011-Present | Cultivation rebounds, leading to record highs in 2017; Afghanistan dominates global production of illicit opium. |
Source: Global Challenges Research Fund[72]
IV. Theory and Intuition
These two phenomena, the American opioid crisis and Afghan opium cultivation, could not seem more separate to some. How can what happens on the streets of American suburbia possibly be tied to what impoverished farmers halfway across the world do? And especially so, when considering that less than one percent of our opium here in the United States is from their collective yield there in Afghanistan?
The key assertion of this paper is that Afghan opium cultivation has contributed to recent declines in prescription opioid and heroin prices in the United States, thereby making these opioids more accessible to the general public and causing more deaths. With this relationship in mind, it is concluded that Afghan opium cultivation negatively impacts, and exacerbates, the American opioid epidemic.
Figure 3. Causality Being Proposed

This serves to confirm a pronounced concern of American drug enforcement officials. According to the BBC News in an article assessing the Trump Administration’s Afghanistan policy:
Afghanistan is by far the biggest producer of opium in the world. According to the US military, 90% of the world’s heroin is made from opium grown in Afghanistan. It makes up 95% of the market in Europe; 90% of the Canadian market. Perhaps surprisingly, Afghan heroin is reckoned to make up only a tiny fraction of the US market. The US Drug Enforcement Agency claims as little as one per cent of US supply is from Afghanistan. It says virtually all the heroin used in America comes from Mexico and South American countries. But, as with any commodity, if there’s more of it on the market, the cost will fall, and US drug enforcement was growing afraid that burgeoning production in Afghanistan would increase world supply and push prices down, making it even more accessible to Americans.[73]
A necessary assumption made in this paper’s contention is that an increase in opioid death rates are a direct consequence of increased opioid consumption as opposed to changes in purity. Indeed, research by Unick et al.[74] found no association between purity and heroin overdose.
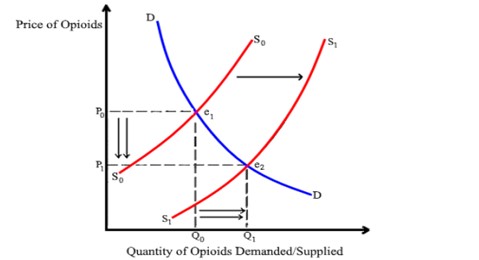
In the context of economic theory, this argument can be depicted through a standard supply and demand model,[75] in which an increase in the global opium supply leads to a rightward shift in opium derivatives’ (i.e., prescription opioids’ and heroin’s) respective supply curves. At the new equilibrium, the lower price leads to a higher quantity demanded . Again, applied to opioids, an increase in per-capita deaths can be inferred from such a rise in demand.
Figure 4. Rightward Supply Shift
Criticisms to this argument do exist though. In November 2017, for instance, Dr. Vanda Felbab-Brown of the Brookings Institution published an article entitled “Afghanistan’s Opium Production is Through the Roof – Why Washington Shouldn’t Overreact.”[76] Among her key arguments were that most American heroin comes from Latin American countries, and very little from Central Asia, and that overdose deaths nowadays are primarily caused by fentanyl overdose via Chinese suppliers. Dr. Felbab-Brown concludes that counternarcotics efforts ought to begin with sustained security, and a more rural-focused Afghan domestic policy that will encourage poppy growers to abandon the practice. In essence, she contends an absence of causality between Afghan opium and American opioid abuse.
However, to suggest that Afghanistan’s meager exports of poppy to the U.S. alone do not impact the epidemic, would also imply that if Afghan opium disappeared overnight (as it nearly did in 2001), opioid consumption across America would be at exactly the same levels. Instead, while barriers to trade indeed do exist (as can be expected in the trade of illegal drugs), consistent with standing economic theory and research, Afghanistan’s opium interacts within a globalized market economy. Dr. Felbab-Brown rules out direct effects on the progression of the American opioid crisis, but ignores the price channels and indirect effects at work throughout the whole of the global market. For example, if Afghan production were to dry up, then markets like those of Canada and western Europe would demand more opium from former U.S. suppliers such as Colombia. This then necessarily drives up the price of opium throughout the western world (including the U.S.), and this fundamentally is the way in which Afghan opium cultivation has impacted the state of the American opioid crisis.
V. Literature Review
There exists a variety of past literature concerning different aspects of the scope of this paper, including that of opioids’ use as substitutes; the price elasticity of demand in opioids; supply-side factors in the American opioid crisis; and outside factors in the opioid crisis.
Opioids as Substitutes
Relating to what will be the first stage of the instrumental variable regression model, a correlation will be demonstrated between the production of Afghan opium and the price of American opioids. One key concern in this contention’s criticisms is the absence of Afghan opium turning into prescription opioids; drugs like oxycodone often utilize their derived opium from nations like Turkey or India,[77] so why does Afghan illicit opium depress Rx opioid prices a hemisphere away, in a nation that almost wholly does not consume its product?
Simply put, the answer is that opioids compete with one another. Given the similarities of effects between the drugs,[78] a dealer of abused prescription opioids must compete, even indirectly, with smuggled heroin and fentanyl for consumers. Fentanyl though is less of a direct “player” in this market, given that much of its consumption is unintentional and not based on consumer-centered decisions.[79]
Substitution among drugs is not uncommon, and has a demonstrated prevalence even among drugs as disparate as alcohol and marijuana.[80] Within the purview of this paper, the substitutability of different iterations of opioids must be demonstrated, so as to further emphasize that Afghan opium impacts the entire opioid market.
The greatest event in which the substitutability of prescription opioids and heroin were noticeable was certainly the April 2010 reformulation of OxyContin (also discussed in Introduction), whereby a mass exodus from Rx to heroin use rapidly took place. Alpert et al.[81] concurred, utilizing difference-in-differences methods to “exploit cross-state variation … isolating the causal relationship between reformulation and heroin deaths.” Evans et al.[82] went further in concluding that “[t]he reformulation did not generate a reduction in combined heroin and opioid mortality [as] each prevented opioid death was replaced with a heroin death.” They found the time at which prescription opioid consumption began falling to be August 2010, with heroin deaths beginning to rise the following month. The neuropharmacological similarities between the two opioid derivatives,[83] combined with heroin’s ease of access and low prices,[84] indeed made heroin an effective substitute for beleaguered prescription opioid addicts.
According to Dr. Jeffrey Singer of the Cato Institute:
[N]on‐medical users of OxyContin can still swallow the ADF OxyContin to get the desired effect. And if the non‐medical users preferred the effect of snorting or injecting the drug, they can readily shift to cheaper and more available heroin (and now also fentanyl). In fact, the evidence shows that is exactly what happened. The ADF formulation had the unintended consequence of driving non‐medical users to more dangerous opioids easily obtainable in the black market. If anything, ADFs grow the overdose rate this way.[85]
In Deiana et al.’s research,[86] the degree of correlation between Afghan farm-gate opium prices and American Rx opioid dispensation was found to be stronger pre-2010 (though still present post-2010), when non-reformulated prescription opioids defined the submarket. All in all, it is strongly evident that different types of opioid are substitutes for one another, and that through this cross-opioid competition, an increase in Afghan opium which typically becomes black tar heroin[87] in turn depresses the price of prescription opioids and fentanyl as well.
Price Elasticity of Demand in Opioids
According to the National Institute on Drug Abuse,[88] the accessibility of a drug is a defining factor in its popularity, and in few places is this more prevalent than the prescription opioid and heroin crises going on in recent years. Furthermore, like many other goods and services in an economy, price is a defining factor in assessing a commodity’s availability. These concepts relate to this paper’s second stage regression, demonstrating correlation between U.S. opioid prices and overdose deaths, with the latter being measured by the CDC and taken as a proxy for consumption overall.
The plethora of past research onhand very much confirms this necessary assumption. While much literature corroborates the existence of a price elasticity of demand in heroin, estimates vary between short and long runs, countries, years, dependency levels, methodologies, and data sources.[89]
The price elasticity of heroin is not an entirely new concept; so long as there was a market, there was an accompanying and noticeable demand elasticity. van Ours[90] took advantage of the Dutch government’s 20th-century monopoly on opium in present-day Indonesia, and found between 1923 and 1938 a short term elasticity of -0.7, and a long term unit elasticity of -1.0. Examining Japanese colonial market-interventions in Taiwan, Liu et al.[91] found between 1914 and 1942 short- and long-run elasticities of -0.48 and -1.38, respectively.
Survey data has been similarly informative, consistently matching theory with practice. Utilizing surveys from Detroit in 1976, Silverman and Spruill[92] found that a 50% increase in the price of heroin led (along with a 14% increase in property crimes) 13% decrease in quantity consumed. Examining both cocaine and heroin price elasticities across twelve U.S. cities between 1987 and 1991 for the Department of Justice, Caulkins[93] concluded that a one percent increase in the U.S. heroin price led to a 1.5 percent decrease in amounts demanded; in other words, that price elasticity was -1.5. Taking a nationwide DEA household survey of 49,802 individuals (N=49,802) , Saffer and Chaloupka[94] gave an estimate of elasticity between -.90 and -0.80.
According to a laboratory (i.e., artificial and controlled) study (N=40) by Petry and Bickel,[95] “[r]eductions in heroin purchases were proportionally less than price increases [between -0.87 and -1.30], demonstrating inelastic demand for heroin.” Interestingly, they also found that an increase in heroin price made user entry into addiction treatment more likely. A decade later, Jofre-Bonet and Petry[96] determined that elasticity remained, albeit varied when considering polydrug use (such as cocaine addicts’ demand for heroin, etc.). Chalmers et al.[97] found elasticities (N=101) above any previously mentioned study, along with differences (between -1.54 and -1.70) based on existing drug dependency levels.
Attempting to count for potential differences due to “hardcore users” via panel data methodology, Dave[98] still determined an elasticity of -0.10. Later, Bretteville-Jensen and Biørn[99] pair conducted two year-apart interviews with participants (N=171) at an Oslo needle exchange, estimating a dealer elasticity between -0.15 and -1.51, and a non-dealer elasticity between -0.71 and -1.69. Roddy and Greenwald[100] argued through interviews (N=100) a price elasticity of -0.64, along with an income elasticity of 0.75. Conducting interviews (N=2,882), Bretteville-Jensen[101] argued -0.77. Finally, Olmstead et al.[102] utilized at the time newly-constructed data, matching surveys with controlled laboratory scenarios and finding an elasticity of -0.80. Appendix A depicts the great majority of standing literature’s elasticity values, as reported by the Council of Economic Advisors.[103]
Prescription opioids are much more complex in that cost-sharing structures like insurance play a role when purchasing legal drugs, and help via income elasticities of demand.[104] Specific to opioids, Powell et al.[105] considered the increased tendency to purchasing- and abuse-risk brought on by Medicare Part D.
Despite this slight evidence pointing to the positive relationship between income and quantity demanded, this should not be interpreted as a counterweight to the negative relationship between price and quantity demanded. Indeed, both often exist in tandem in the market process. The only standing research on prescription opioid price elasticity that could be found is the calculation via crowdsourcing of Strickland et al.,[106] finding a value of -0.62.
The idea that the law of demand applies to fentanyl in a similar way to Rx opioids or heroin is doubtful. As examined by Mars et al., it was determined that:
Current evidence points to a supply-led addition of fentanyl to the drug market in response to heroin supply shocks and shortages, changing prescription opioid availability and/or reduced costs and risks to suppliers. Current drug users in affected regions of the United States, Canada and Europe appear largely to lack both concrete knowledge of fentanyl’s presence in the drugs they buy and access to fentanyl-free alternatives.[107]
This necessitates that any potential similar treatment of fentanyl in future studies be conducted with a grain of salt; drug addicts are still risk-assessing agents who by and large may not want to assume such an astronomically high chance of overdose.[108]
Supply-Side Factors in the U.S. Opioid Crisis
In 2014, Unick et al.[109] used Metropolitan Statistical Area (MSA) data from the DEA and found a correlation between a $100 increase in the price of heroin and a 2.9% increase in overdose hospitalizations, while also determining that a ten percent increase in the market share of Colombian heroin was associated with 4.1% increased hospitalizations. While they focused on the market share of Colombian heroin, this study of course focuses on the growth of the world’s most prolific opium supplier, Afghanistan, following similar theory.
The closest published research that relates to the scope of this paper however is likely that of Deiana et al.[110] They found that from 2003 to 2016, reductions in the farm-gate price of Afghan dry opium led to significant quarterly, county-level increases in the quantity of U.S. prescription opioids dispensed per capita. Similar corresponding increases were found in overdose rates and drug crimes. They wrote that “while we do not claim that pharmaceutical companies make use of raw opium sourced illicitly, we provide suggestive evidence that the shocks in the illicit opium price as measured in Afghanistan are correlated with incentives for the diversion of raw opium from the legal to the illegal market.”[111] Afghan opium prices were interpreted in the paper “as a proxy for world opium prices, because in the last few decades Afghanistan has been the world’s leading producer of illicit opium.”[112] In other words, so goes Afghanistan, so goes the rest of the world. Their paper takes as assumption what this paper intends to further demonstrate: the prevalence of the Afghan opium trade in both global opioid prices, and consequential public health.
In addition, global opium production regularly and substantially exceeds demand. This has led to stockpiles, which, according to some experts, were created explicitly to lessen or counteract depressions in price.[113] While recent and current heroin crises in China, Russia, and India are all seen as primarily Afghan-caused,[114] as well as the city of Kabul internally,[115] such causality is not widely recognized among Americans.
More specifically, according to the United Nations Office on Drugs and Crime:
An anomalous but widely known fact is that, since 2006, much more opium has been produced in Afghanistan than is consumed worldwide … [T]here is now an unaccounted stockpile of 12,000 tons of Afghan opium – enough to satisfy more than two years of world heroin demand … A final anomaly concerns the illicit drug trade and consumption: the numbers just do not add up. For instance India, despite having 800,000 addicts, does not report any inflow of raw opium: either vast quantities of domestic (licensed) production are diverted, opium poppy is being cultivated illicitly in India, or some of the Afghan opium is reaching the subcontinent.[116]
Afghan opium typically becomes black tar heroin.[117] The subsequent cheapness and availability of heroin throughout the world forced prescription opioid smugglers and dealers to offer lower prices (especially as their supply was obstructed by OxyContin’s reformulation). This is the channel through which Afghan opium is able to influence both prescription opioid and heroin-related deaths across the globe.
According to Olcott and Udalova Zwart, “the decreasing price of heroin [in Central Asia] can be explained by both an increased supply of the drug and by the desire of drug dealers to create as many addicts as possible before hiking up the price and making enormous profits.”[118] Therefore, falling prices and increasing demand are recognized by smugglers and dealers as the main profit potential with which they may keep producing poppy.
Interconnectedness of Transnational Opiate Markets
Afghanistan’s vast opium trade has a presence in all of the world opium market, even regions where it maintains only a nominal presence. This is consistent with the economic concept of the gravity equation,[119] wherein trade between two nations is a direct function of their respective gross domestic products, geographic distance, and a constant multiple value reflecting barriers and cultural connections.[120]
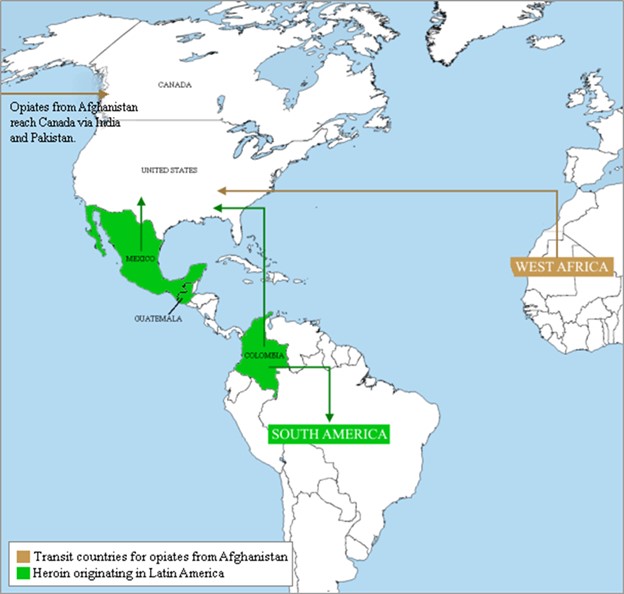
Figure 5 details heroin trafficking from Asia. Per the gravity model, Afghanistan indeed appears to send more heroin to Asian and European nations at a nearer distance.[121] However, the United States and Canada are still mentioned as receiving nations, with Pakistan and India/South Asia as transit regions for both.
According to Rosenblum et al:
The drop in Southwest Asian heroin’s US market share may be due to Afghanistan filling the void in Europe and Asia left by the large decline in Southeast Asian heroin. Once Asian heroin left the US market and their trafficking routes were reduced, there could also be substantial barriers to re-entry. Within the context of our model of market entry, we would assume that the fall in the US market share of Southwest Asian heroin since the early 1990s is due to an inability to compete with the lower cost of Colombian-sourced heroin.[122]
Somewhat contrary to their assertion, this paper instead contends that geographic distance and sparse amounts of consumer-nations do not render insignificant the vast amounts of Afghan opium smuggled across the world every year, and that price channels and the substitutability of opioids indeed do allow for a rightward supply shift to take place.
As Figure 5 shows, most legal American opium comes from India, Australia, France, and Turkey.[123] With reviewed literature onhand, emphatically affirming the means by which people can easily switch between prescription opioids and heroin as competing substitutes, Afghan opium can through these connections also lower the prices of legal, prescribed opioids.
Figure 5. Heroin Trafficking Flows from Asia, 2009
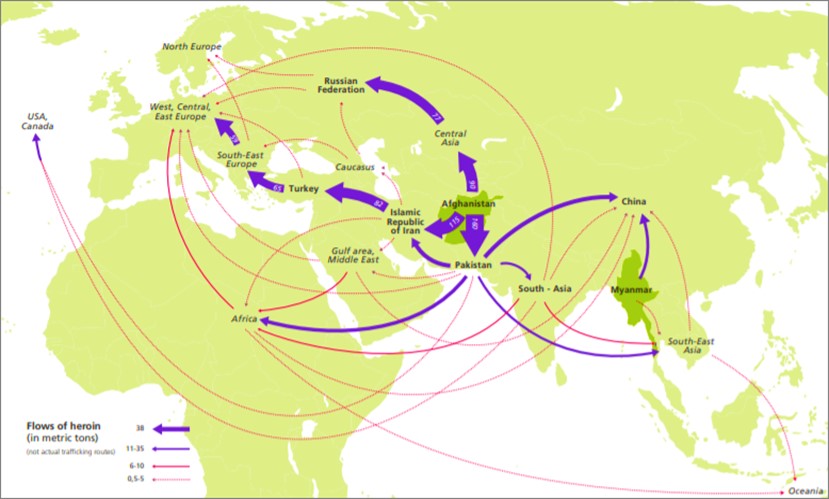
Source: United Nations Office on Drugs and Crime[124]
Figure 6 conversely describes the receipt of heroin and opiates from Afghanistan, Mexico, and South America. While also matching the gravity equation’s intuition regarding opium smuggling from Latin America, this figure interestingly cites West Africa as another transit region. Given that Figure 5 depicts Afghan opium exports in 2009 alone, and Figure 6 shows American/Canadian receipts between 2011 and 2015, it can be concluded that transnational opiate markets are becoming even more connected, having appeared to bring more nations and continents into the fold.
The UNODC expands upon this:
Opium in Afghanistan would be virtually worthless if it could not be sold abroad. Low prices would have prompted Afghan farmers to give up opium production and look for alternative crops. Thus, a link was needed between domestic production and demand for opiates abroad. This link exists due to traders. They have played a crucial role in the growth of Afghanistan’s opiates industry. They developed Afghanistan’s opium market, linking eastern Afghanistan with Pakistan, southern Afghanistan with Pakistan and Iran, and western and northern Afghanistan with neighbouring countries of Central Asia. They identified opium as one out of a few commodities, which could be produced in excess of local demand and for which a strong demand existed outside Afghanistan … In return, traders provided the rural opium poppy growing regions with all the goods – i.e. mainly food, other consumer goods as well as arms – they required. As a result Afghanistan was integrated into the global economy, though based on the export of a rather peculiar raw material.[125]
VI. Data
Data were taken from a variety of governmental sources at the national and international levels. Appendix B lists data and provides numerical descriptive statistics in detail.
Opioid Prices
Data on prescription opioid prices in constant dollars per morphine gram equivalent (MGE) are provided by the Food and Drug Administration[126] via a Freedom of Information Act request. While graphs describing price trends were provided in the FDA’s response, specific figures were provided through email by Dr. Casey B. Mulligan, the former chief economist of the White House Council of Economic Advisors within the Executive Office of the President[127] who in turn compiled the data from the 2001 through 2015 iterations of the Department of Health and Human Services’ Medical Expenditure Panel Survey.[128]
Data on the retail price of one pure gram per MGE of heroin over time were mainly obtained from the Drug Enforcement Administration within the Department of Justice, and reported by the United Nations Office on Drugs and Crime.[129]
Prescription opioid and heroin deaths are both considered opioid overdose deaths;[130] see Appendix C for details on all cause-of-death codes categorized as opioid overdose-related.
Figure 6. Global Heroin Flows of Asian Opium, 2011 – 2015
Source: United Nations Office on Drugs and Crime[131]
Afghan Opium Production
Data on Afghan potential opium production levels are taken from the United Nations Office on Drugs and Crime, which has monitored the nation’s opium trade and culture for several decades. The UNODC is largely considered the most reliable source for opium data in the world.[132]
According to a UNODC document that details the methodology and definition of potential drug production studies:
‘Potential’ heroin or cocaine production shows the level of production of heroin or cocaine if the opium or coca leaf were transformed into the end products in the respective producer country. Part of the opium or the coca leaf is directly consumed in the producing countries or in neighbouring countries, prior to the transformation into heroin or cocaine. … These factors are partly taken into account … Similarly, opium consumed in Afghanistan, Iran and Pakistan is not considered to be available for heroin production. As a result, global estimates of ‘potential’ production should be rather close to ‘actual’ production. Moreover, as the transformation ratios used are rather conservative, total ‘potential’ production may well be close to ‘actual’ production of the end products if one takes the de-facto lower amounts available for starting the transformation process into account.[133]
Potential production therefore constitutes a legitimate and descriptive measure of Afghan opium output over time.
Afghan Instability
As a proxy for instability in Afghanistan and the strength of insurgent organizations, data on the number of battle-related deaths were taken through Uppsala University’s Uppsala Conflict Data Program,[134] and reported through the World Bank’s World Development Indicators series.[135]
The World Bank defines battle-related deaths as:
Deaths in battle-related conflicts between warring parties in the conflict dyad [two conflict units that are parties to a conflict]. Typically, battle-related deaths occur in warfare involving the armed forces of the warring parties. This includes traditional battlefield fighting, guerrilla activities, and all kinds of bombardments of military units, cities, and villages, etc. The targets are usually the military itself and its installations or state institutions and state representatives, but there is often substantial collateral damage in the form of civilians being killed in crossfire, in indiscriminate bombings, etc. All deaths—military as well as civilian—incurred in such situations, are counted as battle-related deaths.[136]
Utilizing population data from the United Nations Department of Economic and Social Affairs,[137] values on battle-related deaths in a given year were taken per 100,000 citizens.
Climate
According to Acock et al.,[138] and converting from Celsius to Fahrenheit, the ideal temperature in which to cultivate poppy is between 64.4 and 68 degrees. As the midpoint of this range, 66.2 degrees is a temperature equidistant from these bounds of favorable temperatures. Therefore, extracting the World Bank’s data for average annual temperature, and calculating the value of this temperature’s deviation from 66.2 degrees Fahrenheit, yields a figure depicting the degree to which Afghan climatic conditions over the course of a year are favorable for poppy growth.
Climate data was received through the World Bank’s Climate Change Knowledge Portal. Data were received for the average temperature in Afghanistan per year, 1994 through 2020. (May typically marks the end of the six-month opium season in the country,[139] though slight differences exist between the northern and southern regions.)
In addition, data on Afghan annual precipitation between 1994 and 2020 were also taken from the Climate Change Knowledge Portal.
Macroeconomic Factors
Hollingsworth et al.[140] found unemployment to be an appropriate indicator of macroeconomic influences on the epidemic. Specifically, at the county level, they established a statistically significant positive relationship between the unemployment rate, and overdose-related emergency room visits and deaths. They attribute this to loss of health insurance, as opposed to lower incomes or higher costs. Contoyannis et al.[141] also stipulated that the price elasticity of prescription drugs are often influenced by healthcare access (due to co-pays, premiums, etc.). This further shows the need for a control variable acting as a proxy for healthcare access. These studies necessitate the use of the U.S. unemployment rate as a similar proxy for macroeconomic conditions when examining opioid affordability, and for which data were extracted from the Federal Reserve Economic Database (FRED) within the Federal Reserve Bank of St. Louis.[142]
Deaths
Through the Centers for Disease Control and Prevention’s WONDER database, data were found for death counts. Overdose deaths were identified from data within this database using ICD-10 underlying cause-of-death codes relating to opioids as defined by the Substance Abuse and Mental Health Services Administration.[143] Appendix C expands upon these codes in greater detail. Taking these coded death quantities in appropriate sums, and adjusting for population based on data from the United States Census Bureau, opioid-related death counts were calculated as per hundred thousand population.
VII. Methods
An endogeneity problem may exist in assessments of the demand elasticity of opioids, as they can be directly influenced by Afghan opium. An instrumental-variable regression model is utilized to account for this, whereby the impact of production changes on price is examined, followed by the impact of price changes on overdose death rates. The first-stage regression model thus has the following general specifications:
(1) $$Δ\widehat{Price}_{d,t}=α_0+α_1 ΔOutput_t+α_2 ΔConflict_t+α_3 ΔUn_t+α_4 ΔWave_{d,t}$$
Where for derivative d in year t, ΔOutput is the annual change in the level of Afghan opium production; ΔConflict is the change in battle-related deaths per capita; ΔUn is the change in the U.S. unemployment rate; Wave is a dummy variable equaling 1 in years where that respective opioid d drove the nation’s increase in opioid overdose deaths (i.e., that opioid’s “wave”), and 0 otherwise; and the dependent variable $$Δ\widehat{Price}$$ is the instrumented (predicted) change in the price of opioid derivative d, whether prescription or heroin. All changes are between years t – 1 and t, 1999 through 2018, in logarithmic form.
Subsequently, the following second-stage regression model utilizes the instrumented changes in American opioid prices to predict its price elasticity of demand/relationship to death rates:
(2) $$Δ\widehat{DeathRate}_{d,t}=β_0+β_1 Δ\widehat{Price}_{d,t}+β_2 ΔUn_t+β_3 ΔWave_{d,t}$$
Where $$Δ\widehat{Price}$$ is the instrumented (predicted) change in the price of an opioid, as discussed above; ΔUn and ΔWave constitute the same changes to unemployment and opioid waves; and $$Δ\widehat{DeathRate}$$ is the predicted change in the prescription opioid overdose rate per 100,000 population. Changes are still in logarithmic form, for the same timeframe of 1999 to 2018. These models are estimated by the software Stata, Version 16.1.
VIII. Results and Discussion
Two-Stage Least Squares Regression
The first set of results reported in Table B are those based on the first-stage impact of Afghan opium output on the price of U.S. opioids. R2 indicates the fit of the model, and N is the overall number of observations/years being studied.
Table B. First-Stage Regression Results
| Rx Price | Heroin Price | |
|---|---|---|
| Output | -0.076**
(0.025) |
-0.120*
(0.161) |
| Conflict | -0.091***
(0.027) |
-0.133**
(0.057) |
| U.S. Unemployment | -0.228**
(0.079) |
0.218
(0.219) |
| Wave | -0.043
(0.433) |
0.022
(0.162) |
| R2 | 0.738 | 0.471 |
| N | 18 | 19 |
Standard errors in parentheses. * p < 0.100 ** p < 0.050 *** p < 0.010
As the findings show, despite an incredibly parsimonious dataset, there is strong evidence that a negative relationship exists between output and prices. A one percent increase in Afghan opium production is associated with a 0.076 percent decrease in the price of American prescription opioids, as well as a 0.12 percent decrease in the price of American heroin. An increase in conflict levels is also associated at statistically significant levels with lower derivative prices in both categories, while an increase in the U.S. unemployment rate is associated with a decrease in prescription opioids’ prices only (consistent with the assertion of Hollingsworth et al.[144] that unemployment is a proxy for health insurance access).
If the assertion that increased production leads to lower derivative prices is accepted, then the previously studied viewpoint that instability is tied to an increase in opioid production is further confirmed here. In the case of both prescription opioids and heroin, an increase in battle-related deaths per capita is significantly correlated with a decrease in a respective derivative’s prices. Instability, it has been written, incentivizes farmers to cultivate and smuggle opium in a geopolitical environment with few other reliable options,[145] and the opium growth responds by helping fund insurgent organizations who have sought to destabilize the Afghan government and economy.[146] Afghan instability also fosters confidence in potential growers that they can elude government crop eradication,[147] and leads to underutilized tax revenue that would otherwise foster internal development and deter opium cultivation.[148]
Table C. Second-Stage Regression Results
| Rx Overdose Rate | Heroin Overdose Rate | |
|---|---|---|
| Instrumented Price | -1.601**
(0.692) |
-3.057***
(0.547) |
| U.S. Unemployment | 0.413
(0.281) |
0.661
(0.415) |
| Wave | -0.262*
(0.146) |
0.307
(0.291) |
| R2 | 0.683 | 0.717 |
| N | 18 | 19 |
Standard errors in parentheses. * p < 0.100 ** p < 0.050 *** p < 0.010
In many of the following figures, data points for the years 2000 and 2001 are marked in diamonds; this will be explained later on (see Results and Discussion).
Statistically significant evidence depicts the relationship hypothesized above. Holding all other factors constant, when Afghan opium cultivation is increased by one percent it is associated with an increase of 0.122 percent in prescription opioid overdoses and 0.367 percent in heroin overdoses.[149]
Figure 7. First-Stage Results: The Impact of Production on Rx and Heroin Prices
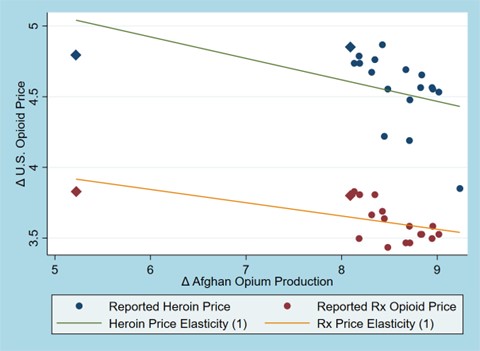
Figure 8. Second-Stage Results; The Impact of Opioid Prices on Overdose Death Rates
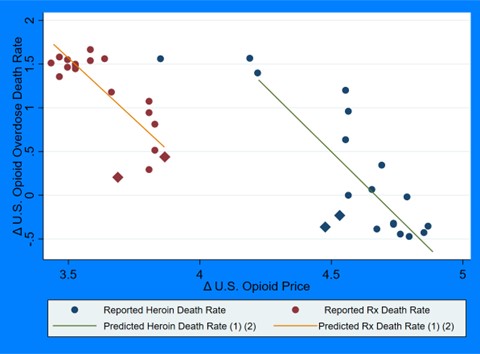
Figure 9. Total Results; The Impact of Afghan Opium Production on U.S. Opioid Overdose Death Rates per 100,000 Population
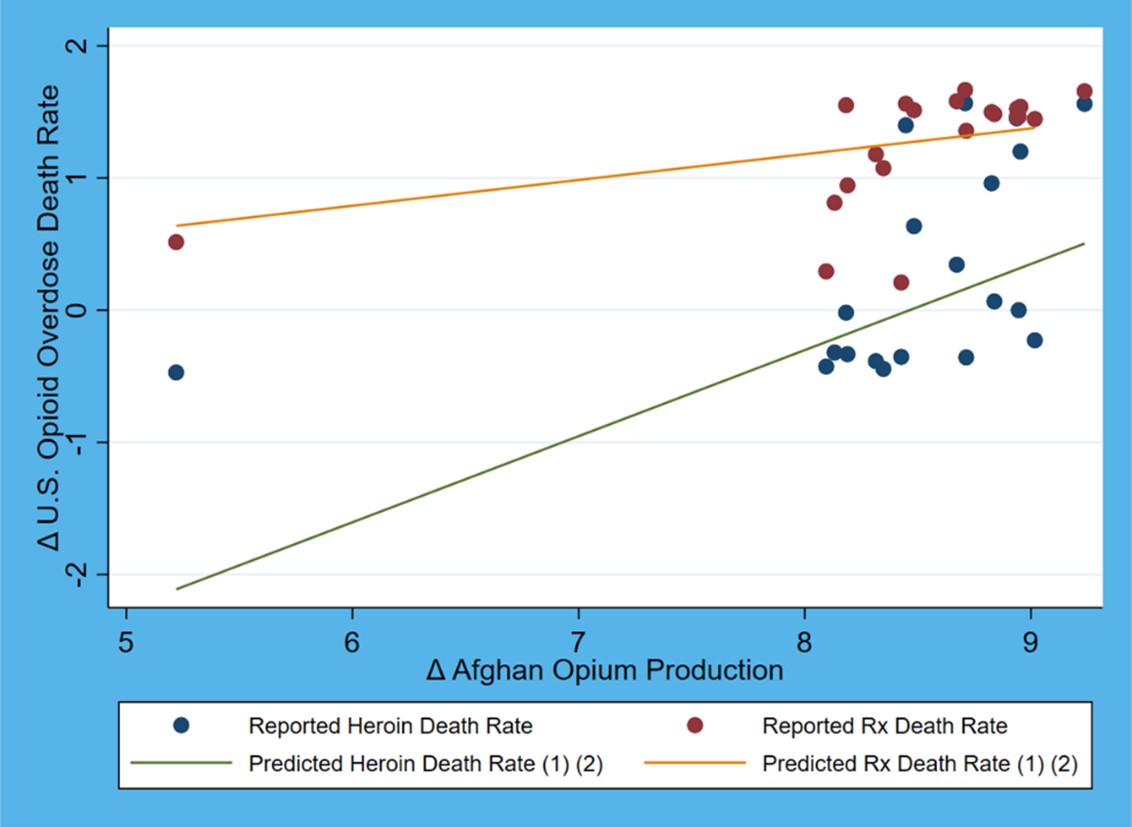
Figure 10. First-Stage Indices
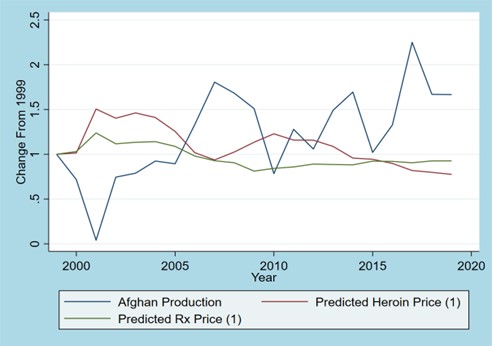
Figure 11. Second-Stage Indices; Rx
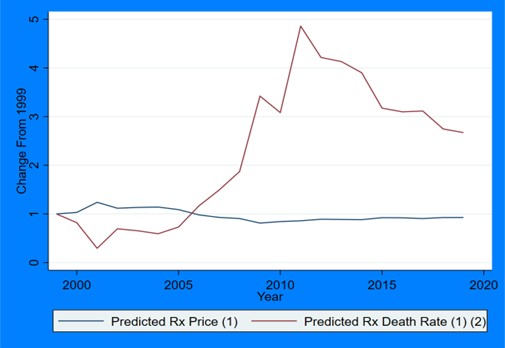
Figure 12. Second-Stage Indices; Heroin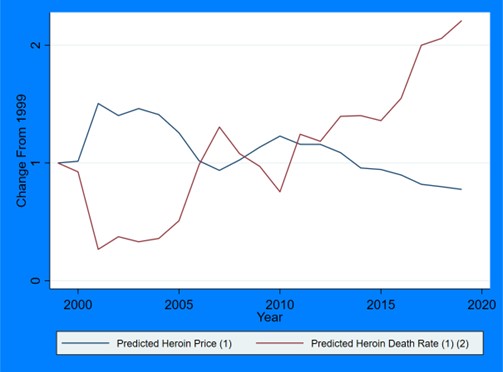
Climatic Supply Shocks
Given that poppies are cultivated plants, with necessary climatic conditions to grow,[150] what then would come of poor weather conditions in the nation? Here this question is addressed, building upon the paper’s above research findings in examining potential ties between Afghanistan’s weather, its opium yield, and U.S. opium derivative prices. It treats poppy yield as a function of two measures with available data, rainfall and temperature, while still including conflict as a proxy for Taliban strength and non-climatic efforts to cultivate opium in the country.[151]
The following model is proposed:
(3) $$Δ\widehat{Output}_t=α_0+ΔTemp_t+α_1 ΔRainfall_t+α_2 ΔConflict_t$$
Where $$Δ\widehat{Output}$$ is the predicted opium output level; ΔTemp is the change in the deviation of annual mean temperature from a midpoint optimal growing temperature, per the research of Acock et al.[152] (see Data); ΔRainfall is the change in annual precipitation in Afghanistan; and ΔConflict is the aforementioned change in population adjusted battle-related deaths, as a proxy for instability which may exogenously affect output. The treatment of temperature data discussed here most directly conflates standing botanical research to consequent opium yield by calculating volatility rather than temperatures alone. Results are depicted in Table D below.
Table D. Climate-Related Regression Results
| Output | |
|---|---|
| Temperature Volatility | -2.878* (1.577) |
| Rainfall | 2.264** 1.007) |
| Conflict | 0.095 (0.156) |
| R2 | 0.299 |
| N | 26 |
Standard errors in parentheses. * p < 0.100 ** p < 0.050 *** p < 0.010
The results depict the American opioid market’s supply shocks brought on by Afghan climate. A one percent increase in temperature volatility appears to decrease output by 2.878 percent, while a one percent increase in precipitation levels there bolsters production levels by 2.264 percent. This is consistent with preconceptions and research on the botanical nature of poppy.
An interesting implication is a potential benefit to climate change. Gümüşçü and Gümüşçü corroborated this by doing more in-depth analysis in Turkey, the world’s leading supplier of legal opium.[153]
As temperatures become more volatile (see Figure 16), and rainfall less prolific, its effect on pernicious crops like illegal drug yields may have a positive impact on certain aspects of global public health. Furthermore, as climate change continues to permeate discussions on global agriculture, therefore, its potential beneficial externalities regarding somewhat-undesirable plants like opium should not go unnoticed.
Figure 13. Causality Between Afghan Climate and American Opioid Overdose Levels

Figure 14. Results; The Impact of Precipitation on Opium Output
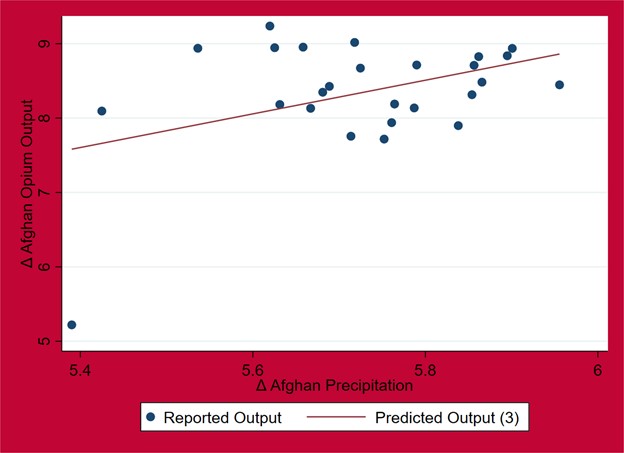
Figure 15. Results; The Impact of Volatile Temperatures on Opium Output
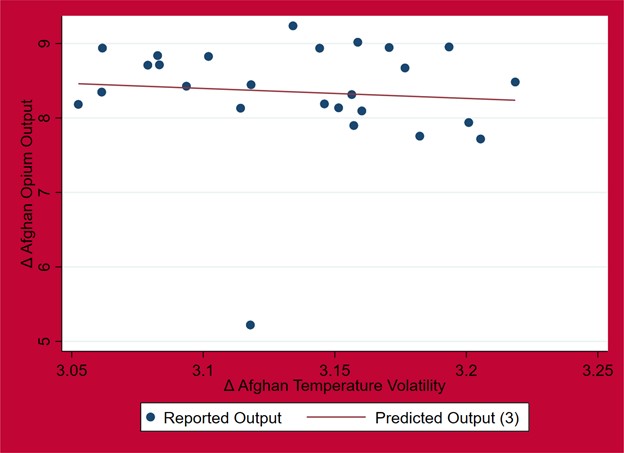
Figure 16. Average Temperature in Afghanistan, 1901-2020
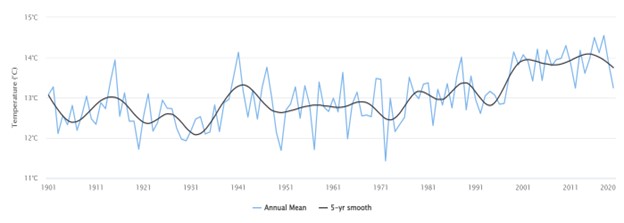
Source: World Bank[154]
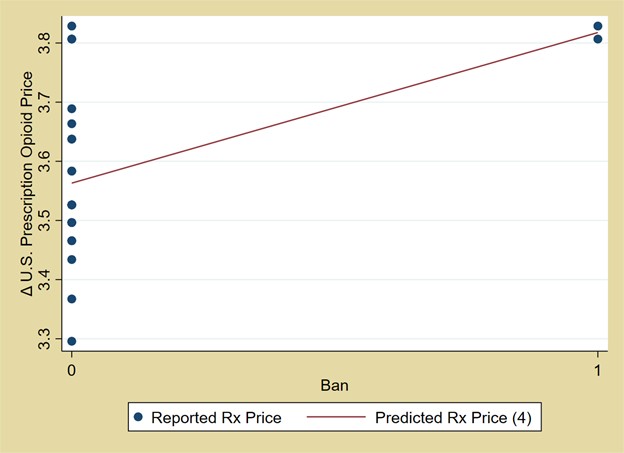
2001 Taliban Opium Ban
As mentioned, between the years 2000 and 2001 the Afghan Taliban instituted and (more importantly) enforced a ban on opium growth. Cultivation levels fell slightly in 2000 and considerably in 2001, before rising back to their pre-ban levels and soon after exceeding them.
The equation below is used to assess the opium ban’s impact on U.S. derivative prices:
(4) $$ΔPrice_{d,t}=α_0+α_1 ΔOutput+α_2 ΔConflict+α_3 ΔUn+α_4 ΔWave+α_5 Ban$$
Where all previously discussed variables from Equation 1 are the same, except that now they also include Ban, a dummy variable equal to 1 for the years 2000 and 2001, the span of time during which the Taliban effectively enforced their ban on opium. Ban is equal to 0 for every other year.
Table E conveys the results. At the 95% confidence level, and holding all other factors constant, the implementation of the Taliban opium ban between years 2000 and 2001 suggests a 23.8 percent increase in the price of U.S. prescription opioids. No impact appears regarding heroin; this is perhaps due to the fact that those two years were in the prescription opioid wave in the U.S., when heroin overall was less used, and for which a wave-specific dummy variable alone can not account.
Such a considerable increase, with such a small dataset, is surprising. However, it is consistent with this paper’s key argument. The restriction of opium in Afghanistan, given their market dominance, effectively raised the price of opium and began a pass-through effect that could be seen in the U.S. medicinal opioid market.
Table E. Ban-Related Regression Results
| Rx Price | Heroin Price | |
|---|---|---|
| Output | -0.007 (0.034) |
-0.251** (0.106) |
| Conflict | -0.135*** (0.025) |
-0.036 (0.074) |
| Un | -0.208** (0.085) |
0.214 (0.308) |
| Wave | -0.104* (0.051) |
-0.092 (0.220) |
| Ban | 0.238** (0.090) |
-0.242 (0.303) |
| R2 | 0.667 | 0.315 |
| N | 23 | 24 |
Standard errors in parentheses. * p < 0.100 ** p < 0.050 *** p < 0.010
Figure 17. The Impact of the Taliban Opium Ban on American Prescription Opioid Prices
“Ban” Years as Outlier Data
Many of the previous figures in the above subsections have featured visible outliers, delineated by diamond symbols. These are the years 2000 and 2001. What then would come of these same regressions when omitting these two years’ data? Equation 1 is used, while this constitution is unchanged; the only alteration has been made in the removal of these two years’ data.
Table F. First-Stage Regression Results Without 2000 or 2001
| Rx Price | Heroin Price | |
|---|---|---|
| Output | -0.135 (0.086) |
-0.190 (0.203) |
| Conflict | -0.087** (0.032) |
-0.123 (0.069) |
| U.S. Unemployment | -0.194** (0.078) |
0.328 (0.223) |
| Wave | -0.053 (0.052) |
0.001 (0.151) |
| R2 | 0.641 | 0.559 |
| N | 16 | 17 |
Standard errors in parentheses. * p < 0.100 ** p < 0.050 *** p < 0.010
When considering the impact of output on prices, in the case of both opioids the models appear to lose statistical significance; based on this truncated data, Afghan opium cultivation would not appear to impact U.S. opioid prices.
The conclusion that follows is that the years 2000 and 2001 helped to typify the indirect relationship at play between Afghan poppy and American overdoses, serving as a pseudo-event study that helps prove the relationship.
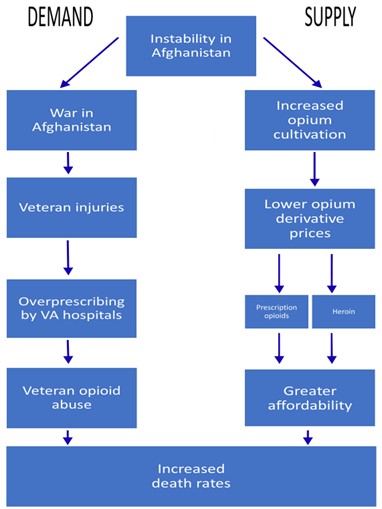
Veteran Opioid Abuse Stemming from the Afghan War
An interesting concept also to be explored in the future is the degree to which Afghan instability, as an instigator of the U.S. War in Afghanistan (2001 – 2021), helped also fuel the American opioid crisis by wounding veterans, to which VA hospitals (as is widely known) have overprescribed opioid painkillers. In other words, Afghanistan may influence demand as well as supply.[155] Figure 18 expands upon this proposed relationship.
At this article’s time of publication, longitudinal data on veteran-specific opioid overdose deaths or abuse rates were not available; as this data continues to become available relative to the proliferation of Afghan opium growth, and particularly so in those two decades during which American service-members fought in Afghanistan, future studies should consider these dual-means of causality between Afghan instability and the U.S. opioid epidemic.
Figure 18. Potential Relationship Relative to Veteran Opioid Abuse
Counterfactuals
If the proposed central argument in this paper is accepted, if there truly is a degree of causality between Afghan opium cultivation and the American opioid epidemic, then any factor impacting the amount of opium grown in Afghanistan would be expected to alter the epidemic’s course as well. All past models suggesting and demonstrating relationships, to that end, are depicted in Figures 20 and 21 with “what-if” counterfactual propositions.
Figure 19. Application of Counterfactual Models; Rx
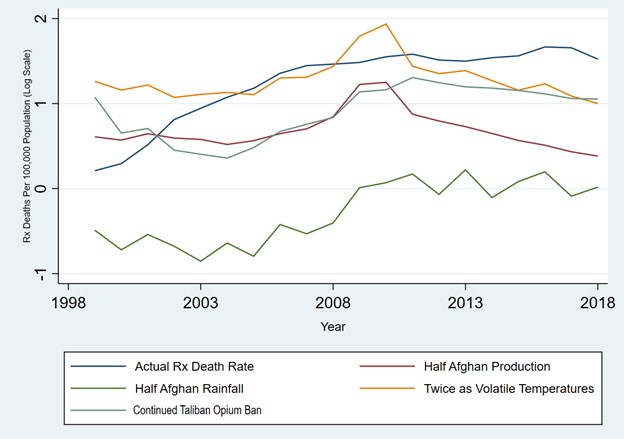
Figure 20. Application of Counterfactual Models; Heroin
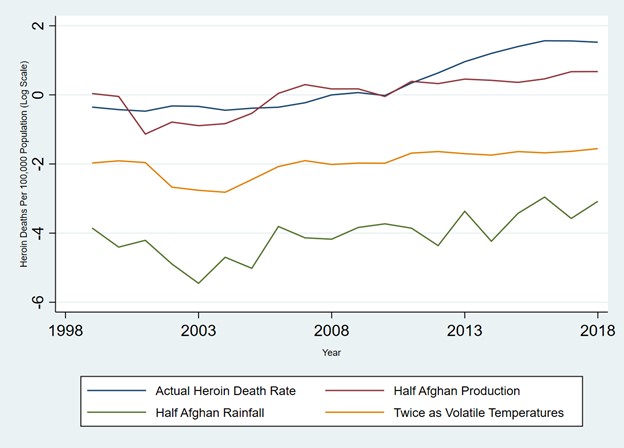
Several projected counterfactual scenarios are evident relative to Afghan opium cultivation’s impact on U.S. public health. In each hypothetical model, a factor that has demonstrated an ability to restrict the Afghan opium supply, and give the global opium market a negative supply shock, had quantifiable implications for opioid overdose levels in America.
The below equation allows the difference in simulated versus real deaths, the projected number of “lives saved,” to be quantified:
(5) $$∑_{t=1999}^{t=2018}[A(t)-C(t)]$$
Where from years t=1999 to t=2018, A(t) is the function depicting actual prescription opioid overdose deaths, and C(t) is a corresponding counterfactual function. The CDC[156] reports a total of 222,825 actual prescription opioid overdose deaths and 111,095 heroin overdose deaths in this timespan.
Of all the counterfactuals, the most impactful on prescription opioids deaths was the doubling of temperature volatility, lowering overdose levels by 78.66% (see Table G).
The illicit heroin market though appears much more susceptible to supply shocks in price when alterations are made to Afghan opium. As shown in Table F, halving Afghan rainfall would make heroin so unaffordable that 98.88 percent of overdose deaths would be avoided. Temperature volatility was similarly impactful, where an Afghan temperature twice as volatile would have cut heroin overdoses by 92.26%.
Limitations
Given that most prescription opioids and heroin directly utilize opium in their production supply chains, and that synthetic opioids by definition do not,[157] the focus of this paper is primarily on changes to the prescription opioid and heroin crises as a result of Afghan cultivation. However, given the capability of competing opioid substitutes and the prevalence of fentanyl,[158]` as data continues to be gathered through methods like online crowd-sourcing methods to eventually create a longitudinal narrative, future studies should consider the role of non-opium opioids in the global supply chain. This relationship may well not exist, as Deiana et al.[159] determined, but warrants further study nonetheless. Examples of such data-gathering methods include the work of Lamy et al.,[160] Miller,[161] Broadhurst et al.,[162] and Dasgupta et al.[163]
In addition, due to annualized values from the UNODC not being able to be parsed into smaller timeframes, and the existence of publicly-available overdose information on the CDC WONDER database beginning only in 1999, this paper lacks a breadth of data for which future studies may hopefully compensate.
Table G. Rx Overdose Counterfactuals Relative to “Lives Saved”
| Projected Death Amount | Projected Number of Lives Saved | Percent Change From Actual | |
|---|---|---|---|
| Half Afghan Opium Production | 111,289.56 | 104,235.1 | -50.06% |
| Continued Taliban Opium Ban | 151,247.66 | 71,577 | -67.88% |
| Twice as Volatile Temperatures | 47,558 | 175,266.89 | -78.66% |
| Half Rainfall | 217,531.02 | 5,293.64 | -2.38% |
Table H. Heroin Overdose Counterfactuals Relative to “Lives Saved”
| Projected Death Amount | Projected Number of Lives Saved | Percent Change From Actual | |
|---|---|---|---|
| Half Afghan Opium Production | 67,803.96 | 43,260.78 | -38.97% |
| Twice as Volatile Temperatures | 8,598.95 | 102,495.79 | -92.26% |
| Half Rainfall | 1,239.77 | 109,854.97 | -98.88% |
IX. Conclusion
The goal of this paper was to assess and quantify how Afghan opium has played a role in, and remains connected to, the ongoing opioid crisis in the United States. From several different angles and perspectives, this has been attempted.
In terms of implications, policymakers going forward may now note the trans-hemispheric underpinnings of the epidemic, as well as how the recent Taliban takeover may impact American public health in the coming years. Domestic treatment alone will not stop the opioid epidemic.[164]
Policies going forward intended to eliminate opium in Afghanistan also should be more nuanced than blind and dogmatic crop eradication, as opium is woven into the modern Afghan way of life[165] and eradication simply increases poverty and anti-government sentiment.[166] Dubious is the idea that Afghan opium can be made legal and join nations like Turkey and India in providing quality anti-pain drugs, particularly due to a lack of financial and political infrastructure to support such an undertaking.[167] However, now having noted the connection between Afghan opium and American opioids in a way not done before, the health-related implications of U.S.-Afghan relations should not go unnoticed.
X. References
Acock, Mary C., Zhongchun Wang, and Basil Acock. “Phases of Development to Flowering in Opium Poppy (Papaver somniferum L.) under Various Temperatures.” Annals of Botany 80, no. 4 (1997): 547-552. https://www.jstor.org/stable/42764942?seq=1#metadata_info_tab_contents.
Ahmed, Azan. “Tasked with Combating Opium, Afghan Officials Profit from It.” The New York Times, February 16, 2016. https://www.nytimes.com/2016/02/16/world/asia/afghanistan-opium-heroin-taliban-helmand.html
Aliprantis, Dionissi, Kyle Fee, and Mark Schweitzer. “Opioids and the Labor Market.” Federal Reserve Bank of Cleveland, November 15, 2019. https://ssrn.com/abstract=3179068.
Alpert, Abby, David Powell, and Rosalie Liccardo Pacula. “Supply-Side Drug Policy in the Presence of Substitutes: Evidence from the Introduction of Abuse-Deterrent Opioids.” Economic Policy 10, no. 4 (2018): 1-35. https://doi.org/10.1257/pol.20170082.
Anderson, James E. “The Gravity Model.” National Bureau of Economic Research (Working Paper 16576), December 2010. https://www.nber.org/papers/w16576.
Bartholet, Jeffrey. “The Holy Men of Heroin.” Newsweek, December 5, 1999. https://www.newsweek.com/holy-men-heroin-163118. Via the Arthur Paul Collection at the University of Nebraska-Omaha.
Basur, Onur, Lin Xie, Jack Mardekian, David Schaaf, Li Wang, and Ashish V. Joshi. “Prevalence of Diagnosed Opioid Abuse and its Economic Burden in the Veterans Health Administration.” Pain Practice 14, no. 5 (2013): 437-445. https://doi.org/10.1111/papr.12097
Becker, Gary S., Michael Grossman, and Kevin M. Murphy. “Rational Addiction and the Effect of Price on Consumption.” The American Economic Review 81, no. 2 (1991): 237-241. https://www.jstor.org/stable/2006861?seq=1#metadata_info_tab_contents.
Bhatia, Jasmine. “Drugs and (Dis)Order in Afghanistan.” Global Challenges Research Fund, April 2020. https://drugs-and-disorder.org/wp-content/uploads/2020/04/Drugs-and-development-in-Afghanistan_Final.pdf
Blanchard, Christopher M. “Afghanistan: Narcotics and U.S. Policy.” Congressional Research Service, August 12, 2009. https://sgp.fas.org/crs/row/RL32686.pdf.
Braner, Sarah. “An Epidemic in the Shadow of a Pandemic: Drug Overdose Deaths Reach an All-Time High in the U.S.” CNN, July 17, 2021. https://www.cnn.com/2021/07/17/health/us-drug-overdose-deaths-pandemic/index.html
Bretteville-Jensen, Anne Linne. “Drug Demand – Initiation, Continuation and Quitting.” De Economist 154, no. 4 (2006): 491-516. https://link.springer.com/article/10.1007/s10645-006-9027-9
Bretteville-Jensen, Anne Linne, and Erik Biørn. “Heroin Consumption, Prices and Addiction: -Evidence from Self-Reported Panel Data.” The Scandinavian Journal of Economics 105, no. 4 (2003): 661-679. https://www.jstor.org/stable/3441136.
Broadhurst, Roderic, Matthew Ball, and Harshit Trivedi. “Fentanyl Availability on Darknet Markets.” Trends and Issues in Crime and Criminal Justice (2020): 790. https://autopapers.ssrn.com/sol3/papers.cfm?abstract_id=3545072
Bureau of International Narcotics and Law Enforcement Affairs. “International Narcotics Control Strategy Report.” U.S. Department of State, March 2, 2021. https://www.state.gov/2021-international-narcotics-control-strategy-report/.
Byrd, William A., and Olivier Jonglez. “Prices and Market Interactions in the Opium Economy.” World Bank / The United Nations, 2006. Via the Arthur Paul Collection at the University of Nebraska-Omaha.
Calabresi, Massimo. “Why America Can’t Kick its Painkiller Problem.” Time, June 4, 2015. https://time.com/3908648/why-america-cant-kick-its-painkiller-problem/
Caulkins, Jonathan P. “Estimating Elasticities of Demand for Cocaine and Heroin with Data from the Drug Use Forecasting System.” United States Department of Justice, 1995. https://www.icpsr.umich.edu/web/NACJD/studies/6567/publications.
Center for Advanced Defense Studies. “Opium in Afghanistan: Lawlessness Thrives on Narcotics Trade.” June 2006. https://www.files.ethz.ch/isn/26992/07_opium_afghan.pdf.
Centers for Disease Control and Prevention. “Understanding the Epidemic.” U.S. Department of Health and Human Services, 2021. https://www.cdc.gov/opioids/basics/epidemic.html.
Cesur, Resul, Joseph J. Sabia, and W. David Bradford. “Did the War on Terror Ignite an Opioid Epidemic?” National Bureau of Economic Research (Working Paper 26264), September 2019. https://www.nber.org/papers/w26264.
Chalmers, Jerry, Deborah Bradford, and Craig Jones. “The Effect of Methamphetamine and Heroin Price on Polydrug Use: A Behavioural Economics Analysis in Sydney, Australia.” International Journal of Drug Policy 21, no. 5 (2010): 381-389. https://doi.org/10.1016/j.drugpo.2010.06.002
Cheng, Hui, and Paul M. Copland. “Incidence of Nonmedical Use of OxyContin and Other Prescription Opioid Pain Relievers Before and After the Introduction of OxyContin with Abuse Deterrent Properties.” Postgraduate Medicine 130, no. 6 (2018): 568-574. https://pubmed.ncbi.nlm.nih.gov/29978755/.
Christie, Chris, Charlie Baker, Roy Cooper, Patrick J. Kennedy, Bertha Madras, and Pam Bondi. “The President’s Commission on Combating Drug Addiction and the Opioid Crisis.” Trump White House Archives, 2017. https://www.doh.wa.gov/Portals/1/Documents/2300/2017/PresidentsCommissionOnCombatingDrugAddictionOpioidCrisis.pdf
Ciccarone, Daniel. “The Triple Wave Epidemic: Opioids, Heroin, and Fentanyl.” Lecture at the University of California-San Francisco, San Francisco, CA, August 19, 2019. https://www.youtube.com/watch?v=iEfjz882rus.
Cicero, Theodore J., Matthew S. Ellis, Hilary L. Surratt, and Steven P. Kurtz. “The Changing Face of Heroin Use in the United States: A Retrospective Analysis of the Past 50 Years.” JAMA Psychiatry 71, no. 7 (2014): 821. https://pubmed.ncbi.nlm.nih.gov/24871348/.
Comer, Sandra D., Maria A. Sullivan, Robert A. Whittington, Suzanne K. Vosburg, and William Kowalcyzk. “Abuse Liability of Prescription Opioids Compared to Heroin in Morphine-Maintained Heroin Abusers.” Neuropsychopharmacology 33, no. 5 (2008): 1179-1191. https://pubmed.ncbi.nlm.nih.gov/17581533/.
Compton, William D., Christopher M. Jones, and Grant T. Baldwin. “Relationship Between Nonmedical Prescription Opioid Use and Heroin Use.” The New England Journal of Medicine 374 (2016): 154-163. https://www.nejm.org/doi/full/10.1056/nejmra1508490.
Contoyannis, Paul, Jeremiah Hurley, Paul Grootendorst, Sung-Hee Jeon, and Robyn Tamblyn. “Estimating the Price Elasticity of Expenditure for Prescription Drugs in the Presence of Non-Linear Price Schedules: An Illustration from Quebec, Canada.” Health Economics 14, no. 6 (2005): 909-923. https://doi.org/10.1002/hec.1041.
Council of Economic Advisors. “The Role of Opioid Prices in the Evolving Opioid Epidemic.” Trump White House Archives, 2019. https://https://trumpwhitehouse.archives.gov/wp-content/uploads/2019/04/The-Role-of-Opioid-Prices-in-the-Evolving-Opioid-Crisis.pdf
Crost, Benjamin, and Santiago Guerrero. “The Effect of Alcohol Availability on Marijuana Use: Evidence from the Minimum Legal Drinking Age.” Journal of Health Economics 31, no. 1 (2012): 112-121. https://doi.org/10.1016/s0167-6296(01)00102-3.
Crow, David. “How Purdue’s ‘One-Two’ Punch Fuelled the Market for Opioids.” Financial Times. September 9, 2018. https://www.ft.com/content/8e64ec9c-b133-11e8-8d14-6f049d06439c
Dasgupta, Nabarun, Clark Freifeld, John S. Brownstein, Christopher Mark Menone, Hilary L. Surratt, Luke Poppish, Jody L. Green, Eric J. Lavonas, and Richard C. Dart. “Crowdsourcing Black Market Prices for Prescription Opioids.” Journal of Medical Internet Research 15, no. 8 (2013): e178. https://pubmed.ncbi.nlm.nih.gov/23956042/.
Dave, Dhaval. “Illicit Drug Use Among Arrestees, Prices and Policy.” Journal of Urban Economics 63, no. 2 (2008): 694-714. https://www.sciencedirect.com/science/article/abs/pii/S0094119007000654.
Deiana, Claudio, Ludovica Giua, and Roberto Nisticó. “The Economics Behind the Epidemic: Afghan Opium Price and Prescription Opioids in the U.S.” IZA Institute of Labor Economics, Discussion Paper Series No. 12872, 2019. https://ftp.iza.org/dp12872.pdf.
DiNardo, John E., and Thomas Lemieux. “Alcohol, Marijuana, and American Youth: The Unintended Effects of Government Regulation.” Journal of Health Economics 20, no. 6 (2001): 991-1010. https://doi.org/10.1016/s0167-6296(01)00102-3.
Drake, Jasmine, Creaque Charles, Jennifer W. Bourgeois, Elycia S. Daniel, and Melissa Kwende. “Exploring the Impact of the Opioid Epidemic in Black and Hispanic Communities in the United States.” Drug Science, Policy, and the Law 0 (2020): 1-11. https://journals.sagepub.com/doi/pdf/10.1177/2050324520940428
Drug Enforcement Administration. “DEA Issues Carfentanil Warning to Police and Public.” U.S. Department of Justice, September 22, 2016. https://www.dea.gov/press-releases/2016/09/22/dea-issues-carfentanil-warning-police-and-public
———. “Dealer Admits Selling Deadly Fentanyl Laced Pills.”U.S. Department of Justice, September 16, 2019. https://www.dea.gov/press-releases/2019/09/16/dealer-admits-selling-deadly-fentanyl-laced-pills
———. “Fentanyl Flow to the United States.” U.S. Department of Justice, March 6, 2020. https://www.dea.gov/documents/2020/2020-03/2020-03-06/fentanyl-flow-united-states.
———. “Fentanyl.” U.S. Department of Justice, 2021. https://www.dea.gov/factsheets/fentanyl.
———. “National Drug Threat Assessment.” U.S. Department of Justice, 2017. https://www.dea.gov/sites/default/files/2018-07/DIR-040-17_2017-NDTA.pdf.
———. “Synthetic Opioids.” U.S. Department of Justice, 2020. https://www.dea.gov/sites/default/files/2020-06/Synthetic%20Opioids-2020.pdf
Duff, Jonathan H. “Opioid Treatment Programs and Related Federal Regulations.” Congressional Research Service, June 12, 2019. https://sgp.fas.org/crs/misc/IF10219.pdf.
Dupee, Matthew C. “The Narcotics Emirate of Afghanistan: Examining Armed Policies and Their Roles in the Illicit Drug Production and Conflict in Afghanistan 1980-2010.” Master’s thesis. Naval Postgraduate School, 2010. https://www.nps.edu/documents/105988371/107571254/DuPeeNarcoticsEmirateThesis.pdf/0f5fde7e-41bc-47c7-ae66-86cdef1019f9. Via the Arthur Paul Afghanistan Collection at the University of Nebraska-Omaha.
Evans, William N., Ethan M.J. Lieber, and Patrick Power. “How the Reformulation of OxyContin Ignited the Heroin Epidemic.” The Review of Economics and Statistics 101, no. 1 (2019): 1-15. https://direct.mit.edu/rest/article-abstract/101/1/1/58660/How-the-Reformulation-of-OxyContin-Ignited-the
Farrell, Graham, and John Thorne. “Where Have All the Flowers Gone?: Evaluation of the Taliban Crackdown Against Opium Poppy Cultivation in Afghanistan.” International Journal of Drug Policy 16, no. 2 (2005): 81-91. https://www.researchgate.net/publication/28576871_Where_have_all_the_flowers_gone_Evaluation_of_the_Taliban_crackdown_against_poppy_cultivation_in_Afghanistan. Via the Arthur Paul Afghanistan Collection at the University of Nebraska-Omaha.
Federal Reserve Bank of St. Louis. “Unemployment Rate.” 2021. https://fred.stlouisfed.org/series/UNRATE/
Felbab-Brown, Vanda. “Afghanistan’s Opium Production is Through the Roof – Why Washington Shouldn’t Overreact.” Brookings Institution, November 21, 2017. https://www.brookings.edu/blog/order-from-chaos/2017/11/21/afghanistans-opium-production-is-through-the-roof-why-washington-shouldnt-overreact/
Felter, Claire. “The U.S. Opioid Epidemic.” Council on Foreign Relations, September 8, 2021. https://www.cfr.org/backgrounder/us-opioid-epidemic
Feng, Emily. “‘We Are Shipping to the U.S.:’ Inside China’s Online Synthetic Drug Networks.” NPR, November 17, 2020. https://www.npr.org/2020/11/17/916890880/we-are-shipping-to-the-u-s-china-s-fentanyl-sellers-find-new-routes-to-drug-user.
Finklea, Kristin. “Heroin Trafficking in the United States.” Congressional Research Service, February 14, 2019. https://sgp.fas.org/crs/misc/R44599.pdf.
Fudin, Jeffrey. “Individual Patient & Medication Factors that Invalidate Morphine Milligram Equivalents.” Presentation at FDA collaborative, June 8, 2021. https://www.fda.gov/media/150393/download.
Galoforo, Claire. “As COVID Fueled the Drug Crisis, Native Americans Hit Worst.” The Associated Press, December 23, 2021. https://apnews.com/article/coronavirus-pandemic-health-minnesota-pandemics-covid-19-pandemic-d2e77c86caa98078248cd6bd75f09150.
Gatwood, Justin, Teresa B. Gibson, Michael E. Chernew, Amanda M. Farr, Emily Vogtmann, and Mark Fendrick. “Price Elasticity and Medication use: Cost Sharing Across Multiple Clinical Conditions.” Journal of Managed Care and Specialty Pharmacy 20, no. 11 (2014): 1102-1107. https://doi.org/10.18553/jmcp.2014.20.11.1102.
Geller, Armando, Seyed M. Mussavi Rizi, and Maciej M. Łatek. “How Corruption Blunts Counternarcotic Policies in Afghanistan: A Multiagent Investigation.” Social Computing, Behavioral-Cultural Modeling, and Prediction 4 (2011): 121-128. https://link.springer.com/content/pdf/10.1007%2F978-3-642-19656-0.pdf. Via the Arthur Paul Afghanistan Collection at the University of Nebraska-Omaha.
Glantz, Aaron. “VA Doctors Tell House Lawmakers of Pressure to Prescribe Veterans Opiates.” Reveal News, October 10, 2013. https://revealnews.org/article/va-doctors-tell-house-lawmakers-of-pressure-to-prescribe-veterans-opiates/.
Goodhand, Jonathan. “From Holy War to Opium War? A Case Study of the Opium Economy in North Eastern Afghanistan.” Disasters 24, no. 2 (2000): 87-102. https://pubmed.ncbi.nlm.nih.gov/10887663/. Via the Arthur Paul Afghanistan Collection at the University of Nebraska-Omaha.
Goodman, J. David. “Naloxone, a Drug to Stop Heroin Deaths, is More Costly, the Police Say.” The New York Times, December 1, 2014. https://www.nytimes.com/2014/12/01/nyregion/prices-increase-for-antidote-to-heroin-overdoses-used-by-police.html.
Grare, Frederic. “Anatomy of a Fallacy: The Senlis Council and Narcotics in Afghanistan.” Carnegie Endowment for International Peace, February 27, 2008. https://carnegieendowment.org/2008/02/27/anatomy-of-fallacy-senlis-council-and-narcotics-in-afghanistan-pub-19937. Via the Arthur Paul Afghanistan Collection at the University of Nebraska-Omaha.
Greenfield, Victoria A., Keith Crane, Craig A. Bond, Nathan Chandler, Jill E. Luoto, and Olga Oliker. “Reducing the Cultivation of Opium Poppies in Southern Afghanistan.” RAND Corporation, 2015. https://www.rand.org/pubs/research_reports/RR1075.html. Via the Arthur Paul Afghanistan Collection at the University of Nebraska-Omaha.
Gümüşçü, Ahmet, and Gönül Gümüşçü. “Climate Change and Effect on Yield Components of Opium Poppy.” Turkish Economic Review 24, no. 1 (2015): 79-84. https://www.biotechstudies.org/uploads/pdf_110.pdf.
Hafvenstein, Joel. Opium Season: A Year on the Afghan Frontier. Guilford: Lyons Press, 2009.
Hagemeier, Nicholas E. “Introduction to the Opioid Epidemic: The Economic Burden on the Healthcare System and Quality of Life.” American Journal of Managed Care 24 (2018): S200-S206. https://pubmed.ncbi.nlm.nih.gov/29851449/.
Hollingsworth, Alex, Christopher J. Ruhm, and Kosali Simon. “Macroeconomic Conditions and Opioid Abuse.” Journal of Health Economics 56 (2017): 222-233. https://pubmed.ncbi.nlm.nih.gov/29128677/.
Hwang, Catherine S., Hsien-Yen Chang, and G. Caleb Alexander. “Impact of Abuse-Deterrent OxyContin on Prescription Opioid Utilization.” Pharmacoepidemiol Drug Safety 24, no. 2 (2015): 197-204. https://pubmed.ncbi.nlm.nih.gov/25393216/.
Inciardi, James A., Hilary L. Surratt, Steven P. Kurtz, and Theodore J. Cicero. “Mechanisms of Prescription Opioid Drug Diversion Among Drug-Involved Club-and-Street-Based Populations.” Pain Medicine 8, no. 2 (2007): 171-183. https://dx.doi.org/10.1111%2Fj.1526-4637.2006.00255.x.
Jofre-Bonet, Mireia, and Nancy Petry. “Trading Apples for Oranges?: Results of an Experiment on the Effects of Heroin and Cocaine Price Changes on Addicts’ Polydrug Use.” Journal of Economic Behavior & Organization 66, no. 2 (2008): 281-311. https://doi.org/10.1016/j.jebo.2006.05.002.
Kolodny, Andrew. “The Opioid Epidemic in 6 Charts.” The Conversation, October 4, 2017. https://theconversation.com/the-opioid-epidemic-in-6-charts-81601.
Lamy, Francois, Raminta Daniulaityte, Monica J. Barrett, Usha Lokala, Amit Sheth, and Robert Carlson. “Listed for Sale: Analyzing Data on Fentanyl, Fentanyl Analogs and Other Novel Synthetic Opioids on One Cryptomarket.” Drug and Alcohol Dependence 213, no. 1 (2010): 108-115. https://doi.org/10.1016/j.drugalcdep.2020.108115.
Larochelle, Marc R., Fang Zhang, Dennis Ross-Degnan, and J. Frank Wharam. “Rates of Opioid Dispensing and Overdose After Introduction of Abuse-Deterrent Extended-Release Oxycodone and Withdrawal of Propoxyphene.” JAMA Internal Medicine 175, no. 6 (2015): 978-987. https://doi.org/10.1001/jamainternmed.2015.0914.
Liddell, David J. “Drugs in Afghanistan: The Challenges With Implementing U.S. Strategy.” Master’s thesis. United States Army War College, March 15, 2008. https://apps.dtic.mil/sti/pdfs/ADA479655.pdf. Via the Arthur Paul Afghanistan Collection at the University of Nebraska-Omaha.
Liu, Jin-Long, Jin-Tan Liu, James K. Hammitt, and Shin-Yi Chou. “The Price Elasticity of Opium in Taiwan, 1914-1942.” Journal of Health Economics 18, no. 6 (1999): 795-810. https://doi.org/10.1016/S0167-6296(99)00023-5.
Los Angeles County Department of Public Health. “Fentanyl.” 2020. http://www.publichealth.lacounty.gov/sapc/managepainsafely/docs/Fentanyl%20FINAL.pdf?pdf=fentanyl.
Luo, Feijun, Mengyao Li, and Curtis Florence. “State-Level Economic Costs of Opioid Use Disorder and Fatal Opioid Overdose.” Morbidity and Mortality Weekly Report 70, (2021): 541-546.http://dx.doi.org/10.15585/mmwr.mm7015a1.
Maclean, Johanna Catherine, Justine Mallatt, Christopher J. Ruhm, and Kosali Simon. “Economic Studies on the Opioid Crisis: A Review.” National Bureau of Economic Research (Working Paper 28067), 2020. https://www.nber.org/papers/w28067.
Manchikanti, Laxmaiah, Sairam Atluri, Hans Hansen, Ramsin M. Benyamin, Frank J.E. Falco, Standiford Helm II, Alan D. Kaye, and Joshua A. Hirsch. “Opioids in Chronic Noncancer Pain: Have we Reached a Boiling Point Yet?” Pain Physician 17, no. 1 (2014): E1-E10. https://pubmed.ncbi.nlm.nih.gov/24452651/.
Mansfield, David, and William Byrd. “Licensing Afghan Opium for Medical Use: Why it Won’t Work.” United States Institute of Peace, September 25, 2014. https://www.usip.org/publications/2014/09/licensing-afghan-opium-medicinal-use. Via the Arthur Paul Afghanistan Collection at the University of Nebraska-Omaha.
Mansfield, David, and Adam Pain. “Alternative Livelihoods: Substance or Slogan?” Afghan Research and Evaluation Unit, October 1, 2005. https://areu.org.af/publication/524/. Via the Arthur Paul Afghanistan Collection at the University of Nebraska-Omaha.
———. “Opium Poppy Eradication: How to Raise Risk When There is Nothing to Lose?” Afghan Research and Evaluation Unit, August 1, 2006. Via the Arthur Paul Afghanistan Collection at the University of Nebraska-Omaha.
Marchildon, Miguel. “An Application of the Gravity Model to International Trade in Narcotics.” Master’s thesis. University of Ottawa, 2018. https://ruor.uottawa.ca/handle/10393/37258.
Mars, Sarah G., Daniel Rosenblum, and Daniel Ciccarone. “Illicit Fentanyls in the Opioid Street Market: Desired or Imposed?” Addiction 114, no. 5 (2018): 774-780. https://pubmed.ncbi.nlm.nih.gov/30512204/.
McCoy, Alfred W. “From Free Trade to Prohibition: A Critical History of the Modern Asian Opium Trade.” Fordham Urban Law Journal 28, no. 1 (2000): 307-349. https://ir.lawnet.fordham.edu/cgi/viewcontent.cgi?article=1804&context=ulj.
Millan, G. Joseph. “Poppy Cultivation in Afghanistan: A Global Strategic Nemesis.” Master’s thesis. United States Army War College, April 7, 2003. https://apps.dtic.mil/sti/citations/ADA414543. Via the Arthur Paul Afghanistan Collection at the University of Nebraska-Omaha.
Miller, Jacob N. “The War on Drugs 2.0: Darknet Fentanyl’s Rise and the Effects of Regulatory and Law Enforcement Action.” Contemporary Economic Policy 38, no. 2 (2019): 246-257. https://doi.org/10.1111/coep.12447.
Miltenburg, John. “Supply Chains for Illicit Products: Case Study of the Global Opiate Production Networks.” Cogent Business & Management 5, no. 1 (2018). https://doi.org/10.1080/23311975.2018.1423871.
Minnesota Department of Health. “Fentanyl Analogs.” 2020. https://www.health.state.mn.us/communities/opioids/basics/fentanyl.html.
Mulligan, Casey B. “Prices and Federal Policies in Opioid Markets.” National Bureau of Economic Research (Working Paper 26812), February 2020. https://www.nber.org/papers/w26812
Nahin, Richard L., Bryan Sayer, Barbara J. Stussman, and Termeh M. Feinberg. “Eighteen-Year Trends in the Prevalence of, and Health Care Use for, Noncancer Pain in the United States: Data from the Medical Expenditure Panel Survey.” Journal of Pain 20, no. 7 (2019): 796-809. https://doi.org/10.1016/j.jpain.2019.01.003.
National Institute on Drug Abuse. “A Subset of People Who Abuse Prescription Opioids May Progress to Heroin Use.” March 17, 2021. https://www.drugabuse.gov/publications/research-reports/prescription-opioids-heroin/subset-users-may-naturally-progress-rx-opioids-to-heroin.
———. “Heroin Use is Driven by its Low Cost and High Availability.” April 13, 2021. https://www.drugabuse.gov/publications/research-reports/prescription-opioids-heroin/heroin-use-driven-by-its-low-cost-high-availability.
———. “Why Does Heroin Use Create Special Risk for Contracting HIV/AIDS and Hepatitis B and C?” April 13, 2021. https://www.drugabuse.gov/publications/research-reports/heroin/why-are-heroin-users-special-risk-contracting-hivaids-hepatitis-b-c.
Niles, Justin K. “The Opioid Epidemic Within the COVID-19 Pandemic: Drug Testing in 2020.” Population Health Management 24 (2021): S43-S51. https://pubmed.ncbi.nlm.nih.gov/33031013/
Office of National Drug Control Policy. “The International Heroin Market.” Obama White House Archives, 2010. https://obamawhitehouse.archives.gov/ondcp/global-heroin-market.
Olcott, Martha B., and Natalia Udalova Zwart. “Drug Trafficking on the Great Silk Road: The Security Environment in Central Asia.” Carnegie Endowment for International Peace, March 1, 2000. https://carnegieendowment.org/2000/03/01/drug-trafficking-on-great-silk-road-security-environment-in-central-asia-pub-292. Via the Arthur Paul Afghanistan Collection at the University of Nebraska-Omaha.
Olmstead, Todd A., Sheila M. Alessi, Brendan Kline, Rosalie Liccardo Pacula, and Nancy M. Petry. “The Price Elasticity of Demand for Heroin: Matched Longitudinal and Experimental Evidence.” Journal of Health Economics 41 (2015): 59-71. https://doi.org/10.1016/j.jhealeco.2015.01.008.
Peters, Gretchen. “How Opium Profits the Taliban.” United States Institute of Peace, August 2, https://www.usip.org/publications/2009/08/how-opium-profits-taliban. Via the Arthur Paul Afghanistan Collection at the University of Nebraska-Omaha.
Petry, Nancy M., and Warren K. Bickel. “Polydrug Abuse in Heroin Addicts: A Behavioral Economic Analysis.” Addiction 93, no. 3 (1998): 321-325. https://doi.org/10.1046/j.1360-0443.1998.9333212.x.
Powell, David, Rosalio Liccardo Pacula, and Erin Taylor. “How Increasing Medical Access to Opioids Contributes to the Opioid Epidemic: Evidence from Medicare Part D.” Journal of Health Economics 71(2020): 102286. https://doi.org/10.1016/j.jhealeco.2019.102286.
Realuyo, Celina B. “The New Opium War: A National Emergency.” Prism 8, no. 1 (2019). https://cco.ndu.edu/Portals/96/Documents/prism/prism8_1/190306_PRISM8_1_Realuyo.pdf?ver=2019-03-05-152931-517.
Roddy, Juliette, and Mark Greenwald. “An Economic Analysis of Income and Expenditures by Heroin-Using Research Volunteers.” Substance Use & Misuse 44, no. 11 (2009): 1502 -1518. https://dx.doi.org/10.1080%2F10826080802487309.
Rosen, Liana W., and Susan V. Lawrence. “Illicit Fentanyl and China’s Role.” Congressional Research Service, January 29, 2021. https://crsreports.congress.gov/product/pdf/IF/IF10890.
Rosenblum, Daniel, George J. Unick, and Daniel Ciccarone. “The Entry of Colombian-Sourced Heroin into the US Market: The Relationship Between Competition, Price, and Purity.” International Journal of Drug Policy 25, no. 1 (2014): 88-95. https://doi.org/10.1016/j.drugpo.2013.10.003.
Rowlatt, Justin. “How the US Military’s Opium War in Afghanistan was Lost.” BBC News, April 25, 2019. https://www.bbc.com/news/world-us-canada-47861444.
———. “What the Heroin Industry Can Teach Us About Solar Power.” BBC News, July 27, 2020. https://www.bbc.com/news/science-environment-53450688.
Ruiz-Goiriena, Romina. “Florida is the Epicenter of the Nation’s HIV and Opioid Crises. This Doctor is Battling to Stop the Virus and Winning.” USA Today, November 17, 2021. https://www.usatoday.com/story/news/nation/2021/11/15/hiv-transmission-doctors-mission-his-unique-plan-pays-off/6238356001/?gnt-cfr=1.
Sacco, Lisa N., Kristin Finklea, Susan V. Lawrence, Liana W. Rosen, and Clare Ribando Seelke. “The Opioid Epidemic: Supply Control and Criminal Justice Policy — Frequently Asked Questions.” Congressional Research Service, June 28, 2019. https://sgp.fas.org/crs/misc/R45790.pdf
Saffer, Henry, and Frank Chaloupka. “The Demand for Illicit Drugs.” Economic Inquiry 37 (2007): 401-411. https://doi.org/10.1111/j.1465-7295.1999.tb01439.x.
Schuchat, Anne, Debra Houry, and Gery P. Guy Jr. “New Data on Opioid Use and Prescribing in the United States.” Journal of the American Medical Association 318, no. 5 (2017): 425-426. https://jamanetwork.com/journals/jama/article-abstract/2643332.
Silverman, Lester P., and Nancy L. Spruill. “Urban Crime and the Price of Heroin.” Journal of Urban Economics 4, no. 1 (1977): 80-103. https://doi.org/10.1016/0094-1190(77)90032-8.
Simmons-Duffin, Selena. “The Real Cost of the Opioid Epidemic: An Estimated $179 Billion in Just 1 Year.” NPR, October 24, 2019. https://www.npr.org/sections/health-shots/2019/10/24/773148861/calculating-the-real-costs-of-the-opioid-epidemic.
Singer, Jeffrey. “Abuse-Deterrent Opioids and the Law of Unintended Consequences.” Cato Institute, February 6, 2018. https://www.cato.org/policy-analysis/abuse-deterrent-opioids-law-unintended-consequences.
———. “The Abuse-Deterrent Folly.” Cato Institute, September 12, 2020. https://www.cato.org/blog/abuse-deterrent-folly.
Smart, Rosanna, Bryce Pardo, and Corey S. Davis. “Systematic Review of the Emerging Literature on the Effectiveness of Naloxone Access Laws in the United States.” Addiction 116, no. 1 (2021): 16-17. https://doi.org/10.1111/add.15163.
Snyder, Edwin F. “War, Drugs, and Money: The Opium Trade in Afghanistan.” Master’s thesis. Harvard University, 2019. https://dash.harvard.edu/handle/1/37365391.
Stevens, Alex. Drugs, Crime and Public Health: The Political Economy of Drug Policy. New York: Routledge, 2011.
Strickland, Justin C., Joshua A. Lile, and William W. Stoops. “Evaluating Non-Medical Prescription Opioid Demand Using Commodity Purchase Tasks: Test-Retest Reliability and Incremental Validity.” Psychopharmacology 236 (2019): 2641-2652. https://doi.org/10.1007/s00213-019-05234-y.
Substance Abuse and Mental Health Services Administration. “Using International Classification of Diseases (ICD) Codes to Assess Opioid-Related Overdose Deaths.” U.S. Department of Health and Human Services (2021). https://mnprc.org/wp-content/uploads/2019/01/using-icd-10-codes-to-assess-opioid-related-overdose-deaths.pdf.
Swartz, Brandon J. “Afghanistan Connection: Heroin Production, Distribution, and Consumption.” Master’s thesis. Michigan Technological University, 2011. https://digitalcommons.mtu.edu/etds/443/.
Thomas, Daniel. “Opioid Crisis: US Pharmacies Face Moment of Truth as Trial Begins.” BBC News, October 6, 2021. https://www.bbc.com/news/business-58820598.
Unick, George, Daniel Rosenblum, Sarah Mars, and Daniel Ciccarone. “The Relationship Between US Heroin Market Dynamics and Heroin-Related Overdose, 1992-2000.” Addiction 109, no. 11 (2014): 1889-1998. https://onlinelibrary.wiley.com/doi/10.1111/add.12664.
United Nations Office on Drugs and Crime. “Afghanistan: Community Drug Profile 5.” The United Nations, July 31, 2003. https://www.unodc.org/pdf/afg/report_2003-07-31_1.pdf. Via the Arthur Paul Afghanistan Collection at the University of Nebraska-Omaha.
———. The Opium Economy in Afghanistan: An International Problem. New York: UNODC, Via the Arthur Paul Afghanistan Collection at the University of Nebraska-Omaha.
———. “Afghan Farmers’ Intentions Survey 2003/2004.” The United Nations, 2004. https://www.unodc.org/pdf/afg/afg_fis_report_2003-2004.pdf. Via the Arthur Paul Afghanistan Collection at the University of Nebraska-Omaha.
———. “Summary Findings of Opium Trends in Afghanistan, 2005.” The United Nations, September 6, 2005. https://www.unodc.org/pdf/afg/2005SummaryFindingsOfOpiumTrendsAfghanistan.pdf. Via the Arthur Paul Afghanistan Collection at the University of Nebraska-Omaha.
———. “Addiction, Crime, and Insurgency: The Transnational Threat of Afghan Opium.” The United Nations, 2009. https://www.unodc.org/unodc/en/data-and-analysis/addiction-crime-and-insurgency.html. Via the Arthur Paul Afghanistan Collection at the University of Nebraska-Omaha.
———. “Afghan Opiate Trafficking Along the Northern Route.” The United Nations, 2018. https://www.unodc.org/documents/publications/NR_Report_21.06.18_low.pdf
———. “The Global Heroin Market.” The United Nations, 2010. https://www.unodc.org/documents/wdr/WDR_2010/1.2_The_global_heroin_market.pdf. Via the Arthur Paul Afghanistan Collection at the University of Nebraska-Omaha.
———. “World Drug Report: Methodology.” The United Nations, 2008. https://www.unodc.org/documents/wdr/WDR_2008/WDR2008_Methodology.pdf.
———. “World Drug Report 2010.” The United Nations, 2010. https://www.unodc.org/documents/wdr/WDR_2010/World_Drug_Report_2010_lo-res.pdf. Via the Arthur Paul Afghanistan Collection at the University of Nebraska-Omaha.
———. “The Global Afghan Opium Trade: A Threat Assessment.” The United Nations, July 20 https://www.unodc.org/documents/data-and-analysis/Studies/Global_Afghan_Opium_Trade_2011-web.pdf. Via the Arthur Paul Afghanistan Collection at the University of Nebraska-Omaha.
———. “Afghan Opium Survey 2019.” The United Nations, 2020. https://www.unodc.org/documents/crop-monitoring/Afghanistan/20210217_report_with_cover_for_web_small.pdf. Via the Arthur Paul Afghanistan Collection at the University of Nebraska-Omaha.
United Nations Department of Economic and Social Affairs. “Annual Total Population at Mid-Year (Thousands).” The United Nations, 2021. https://population.un.org/wup/DataQuery/.
United States Sentencing Commission. “Fentanyl and Fentanyl Analogs.” United States Sentencing Commission, January 25, 2021. https://www.ussc.gov/research/research-reports/fentanyl-and-fentanyl-analogues-federal-trends-and-trafficking-patterns.
Uppsala Conflict Data Program. “Afghanistan.” https://ucdp.uu.se/country/700.
U.S. Congress. House of Representatives. Committee on Energy and Commerce. Fentanyl: The Next Wave of the Opioid Crisis. 115th Cong., 1st sess., March 21, 2017. https://www.youtube.com/watch?v=Ad-8mdZ-rCo.
Van Handel, Michelle M., Charles E. Rose, Elaine J. Hallisey, Jessica L. Kolling, Jon E. Zibbell, Brian Lewis, Michelle K. Bohm, Christopher M. Jones, Barry E. Flanagan, Azfar-E- Alam Siddiqi, Kashif Iqbal, Andrew L. Dent, Jonathan H. Mermin, Eugene McCray, John W. Ward, and John T. Brooks. “County-Level Vulnerability Assessment for Rapid Dissemination of HIV or HCV Infections Among Persons Who Inject Drugs, United States.” Journal of Acquired Immune Deficiency Syndrome 72, no. 3 (2016): 323-321. https://doi.org/10.1097/qai.0000000000001098.
van Ours, Jan C. “The Price Elasticity of Hard Drugs: The Case of Opium in the Dutch East Indies, 1923-1938.” Journal of Political Economy 103, no. 2 (1995): 261-279. https://www.journals.uchicago.edu/doi/abs/10.1086/261983.
Walker, William. Opium and Foreign Policy: The Anglo-American Search for Order in Asia, 1912-1954. Chapel Hill: University of North Carolina Press, 1991.
Wardak, Ali. “Integrated Social Control in Afghanistan: Implications for the Licensed Cultivation of Poppy for the Production of Medicines.” The International Council on Security and Development (2006). https://www.researchgate.net/publication/237387403_Integrated_Social_Control_in_Afghanistan_Implications_for_the_Licensed_Cultivation_of_Poppy_for_the_Production_of_Medicines.
Werb, Daniel, Thomas Kerr, Julio Montaner, and Evan Wood. “The Need for an Evidence-Based Approach to Controlling Opium Production in Afghanistan.” Journal of Public Health Policy 29, no. 4 (2008): 440-448. https://www.jstor.org/stable/40207209.
Wolff, Carolyn, William N. Dowd, Mir M. Ali, Chandler McClellan, Angelica Meinhofer, Lukas Glos, Ryan Mutter, Matthew Rosenberg, and Andreas Schick. “The Impact of the Abuse-Deterrent Reformulation of OxyContin on Prescription Pain Reliever Misuse and Heroin Initiation.” Addictive Behaviors 105 (2020). https://pubmed.ncbi.nlm.nih.gov/32036188/.
World Bank, “Climate Change Knowledge Portal,” 2020. https://climateknowledgeportal.worldbank.org/country/afghanistan/climate-data-historical.
World Bank. “World Development Indicators,” 2019. https://data.worldbank.org/.
Appendices
Appendix A. Estimates of the Price Elasticity of Demand for Heroin (-%)
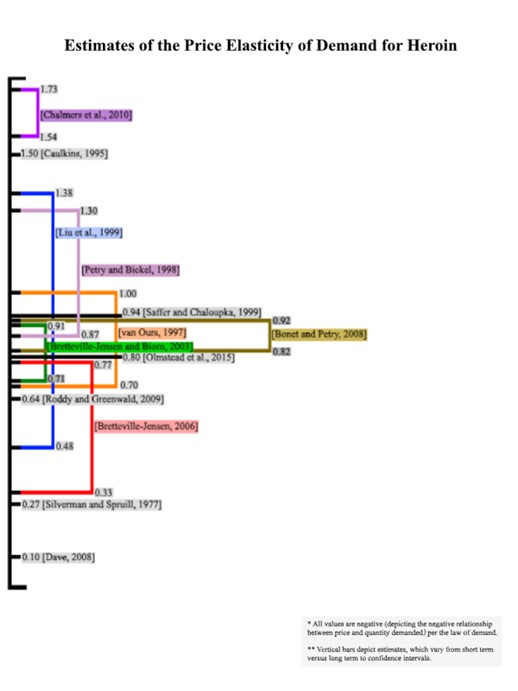
Source: White House Council of Economic Advisors[168]
Appendix B: Descriptive Statistics
| Source | N | Mean | S.D. | Min | 1st Qr | Med | 3rd Qr | Max | |
|---|---|---|---|---|---|---|---|---|---|
| Afghan Mean Temperature | World Bank | 27 | 13.77 | 0.48 | 12.84 | 13.42 | 13.86 | 14.14 | 14.55 |
| Afghan Opium Production | UNODC | 26 | 5,027.54 | 2,351.29 | 185 | 3,400 | 4,612 | 6,891 | 10,270 |
| Afghan Population (Millions) | UN Population Division | 26 | 26.9 | 6.47 | 20.17 | 20.78 | 26.77 | 32.27 | 37.17 |
| Afghan Precipitation Levels | World Bank | 27 | 312.9 | 42.5 | 219.21 | 286.55 | 314.89 | 349.48 | 385.9 |
| Battle-Related Deaths in Afghanistan | Uppsala Conflict Data Program | 26 | 8,647.1 | 7,462.37 | 687 | 4,750 | 6,368.5 | 8,937 | 29,940 |
| Heroin Prices | DEA | 24 | 113.17 | 33.03 | 47 | 95 | 111.5 | 129 | 188 |
| Overdose Deaths; Heroin | CDC | 21 | 6,170.81 | 5,337.87 | 1,779 | 2,080 | 3,041 | 10,574 | 15,482 |
| Overdose Deaths; Rx | CDC | 21 | 11,744.95 | 4,324.91 | 3,442 | 8,577 | 13,523 | 14,838 | 17,087 |
| Rx Opioid Prices | US DHHS | 23 | 36.52 | 5.64 | 27 | 33 | 34 | 40 | 46 |
| U.S. Population (Millions) | US Census Bureau | 26 | 298.56 | 20.17 | 279.04 | 281.16 | 299.81 | 315.99 | 326.69 |
| U.S. Unemployment Rate | Federal Reserve Economic Database (FRED) | 27 | 5.8 | 1.68 | 3.68 | 4.61 | 5.41 | 6.16 | 9.61 |
Appendix C: ICD-10 Cause of Death Codes
| Cause of Death Code | Description | Manner of Death |
|---|---|---|
| X40 | Accidental poisoning by and exposure to non-opioid analgesics, antipyretics and anti-rheumatics | Accidental poisoning |
| X41 | Accidental poisoning by and exposure to antiepileptic, sedative-hypnotic, antiparkinsonism and psychotropic drugs, not elsewhere classified | |
| X42 | Accidental poisoning by and exposure to narcotics and psychodysleptics [hallucinogens], not elsewhere classified | |
| X43 | Accidental poisoning by and exposure to other drugs acting on the autonomic nervous system | |
| X44 | Accidental poisoning by and exposure to other and unspecified drugs, medicaments and biological substances | |
| X60 | Intentional self-poisoning by and exposure to non-opioid analgesics, antipyretics and anti-rheumatics | Intentional self-poisoning (suicide) |
| X61 | Intentional self-poisoning by and exposure to antiepileptic, sedative-hypnotic, anti-parkinsonism and psychotropic drugs, not elsewhere classified | |
| X62 | Intentional self-poisoning by and exposure to narcotics and psychodysleptics [hallucinogens], not elsewhere classified | |
| X63 | Intentional self-poisoning by and exposure to other drugs acting on the autonomic nervous system | |
| X64 | Intentional self-poisoning by and exposure to other and unspecified drugs, medicaments and biological substances | |
| X85 | Assault by drugs, medicaments and biological substances | Assault (homicide) |
| Y10 | Poisoning by and exposure to nonopioid analgesics, antipyretics and antirheumatics, undetermined intent | Poisoning: Undetermined intent |
| Y11 | Poisoning by and exposure to antiepileptic, sedative-hypnotic, antiparkinsonism and psychotropic drugs, not elsewhere classified, undetermined intent | |
| Y12 | Poisoning by and exposure to narcotics and psychodysleptics [hallucinogens], not elsewhere classified, undetermined intent | |
| Y13 | Poisoning by and exposure to other drugs acting on the autonomic nervous system, undetermined intent | |
| Y14 | Poisoning by and exposure to other and unspecified drugs, medicaments and biological substances, undetermined intent | |
| T40.0 | Opium poisoning | Contributing cause of death |
| T40.1 | Heroin poisoning | |
| T40.2 | Other opioids poisoning | |
| T40.3 | Methadone poisoning | |
| T40.4 | Other synthetic narcotics poisoning | |
| T40.6 | Other/unspecified narcotics |
[1] Chris Christie, Charlie Baker, Roy Cooper, Patrick J. Kennedy, Bertha Madras, and Pam Bondi, “The President’s Commission on Combating Drug Addiction and the Opioid Crisis.” Trump White House Archives, 2017; Claire Felter, “The U.S. Opioid Epidemic,” Council on Foreign Relations, September 8, 2021; Justin K. Niles, “The Opioid Epidemic Within the COVID-19 Pandemic: Drug Testing in 2020,” Population Health Management 24 (2021): S43-S51; Sarah Braner, “An Epidemic in the Shadow of a Pandemic: Drug Overdose Deaths Reach an All-Time High in the U.S.,” CNN, July 17, 2021.
[2] Feijun Luo, Mengyao Li, and Curtis Florence, “State-Level Economic Costs of Opioid Use Disorder and Fatal Opioid Overdose,” Morbidity and Mortality Weekly Report 70, (2021): 541-546.
[3] Selena Simmons-Duffin, “The Real Cost of the Opioid Epidemic: An Estimated $179 Billion in Just 1 Year,” NPR, October 24, 2019.
[4] Theodore J Cicero, Matthew S. Ellis, Hilary L. Surratt, and Steven P. Kurtz. “The Changing Face of Heroin Use in the United States: A Retrospective Analysis of the Past 50 Years,” JAMA Psychiatry 71, no. 7 (2014): 821.
[5] Jasmine Drake, Creaque Charles, Jennifer W. Bourgeois, Elycia S. Daniel, and Melissa Kwende, “Exploring the Impact of the Opioid Epidemic in Black and Hispanic Communities in the United States,” Drug Science, Policy, and the Law 0 (2020): 1-11; Claire Galoforo, “As COVID Fueled the Drug Crisis, Native Americans Hit Worst,” The Associated Press, December 23, 2021.
[6] Celina B. Realuyo, “The New Opium War: A National Emergency,” Prism 8, no. 1 (2019).
[7] Dionissi Aliprantis, Kyle Fee, and Mark Schweitzer, “Opioids and the Labor Market,” Federal Reserve Bank of Cleveland, November 15, 2019.
[8] Gary S. Becker, Michael Grossman, and Kevin M. Murphy, “Rational Addiction and the Effect of Price on Consumption,” The American Economic Review 81, no. 2 (1991): 237-241.
[9] Abby Alpert, David Powell, and Rosalie Liccardo Pacula, “Supply-Side Drug Policy in the
Presence of Substitutes: Evidence from the Introduction of Abuse-Deterrent Opioids,” Economic Policy 10, no. 4 (2018): 1-35; National Institute on Drug Abuse, “A Subset of People Who Abuse Prescription Opioids May Progress to Heroin Use,” March 17, 2021; William D. Compton, Christopher M. Jones, and Grant T. Baldwin, “Relationship Between Nonmedical Prescription Opioid Use and Heroin Use,” The New England Journal of Medicine 374 (2016): 154-163.
[10] Casey B. Mulligan, “Prices and Federal Policies in Opioid Markets,” National Bureau of Economic Research (Working Paper 26812), February 2020.
[11] Office of National Drug Control Policy, “The International Heroin Market,” Obama White House Archives, 2010.
[12] Claudio Deiana, Ludovica Giua, and Roberto Nisticó, “The Economics Behind the Epidemic: Afghan Opium Price and Prescription Opioids in the U.S.,” IZA Institute of Labor Economics, Discussion Paper Series No. 12872, 2019.
[13] Richard L. Nahin, Bryan Sayer, Barbara J. Stussman, and Termeh M. Feinberg. “Eighteen-Year Trends in the Prevalence of, and Health Care Use for, Noncancer Pain in the United States: Data from the Medical Expenditure Panel Survey.” Journal of Pain 20, no. 7 (2019): 796-809.
[14] Massimo Calabresi, “Why America Can’t Kick its Painkiller Problem,” Time, June 4, 2015; Nicholas E. Hagemeier, “Introduction to the Opioid Epidemic: The Economic Burden on the Healthcare System and Quality of Life,” American Journal of Managed Care 24 (2018): S200-S206.
[15] Centers for Disease Control and Prevention, “Understanding the Epidemic,” U.S. Department of Health and Human Services, 2021.
[16] Laxmaiah Manchikanti, Sairam Atluri, Hans Hansen, Ramsin M. Benyamin, Frank J.E. Falco, Standiford Helm II, Alan D. Kaye, and Joshua A. Hirsch, “Opioids in Chronic Noncancer Pain: Have We Reached a Boiling Point Yet?,” Pain Physician 17, no. 1 (2014): E1-E10.
[17] Andrew Kolodny, “The Opioid Epidemic in 6 Charts,” The Conversation, October 4, 2017; David Crow, “How Purdue’s ‘One-Two’ Punch Fuelled the Market for Opioids,” Financial Times, September 9, 2018.
[18] Aaron Glantz, “VA Doctors Tell House Lawmakers of Pressure to Prescribe Veterans Opiates,” Reveal News, October 10, 2013; Daniel Thomas, “Opioid Crisis: US Pharmacies Face Moment of Truth as Trial Begins,” BBC News, October 6, 2021.
[19] James A. Inciardi, Hilary L. Surratt, Steven P. Kurtz, and Theodore J. Cicero, “Mechanisms of Prescription Opioid Drug Diversion Among Drug-Involved Club-and-Street-Based Populations,” Pain Medicine 8, no. 2 (2007): 171-183.
[20] Nicholas E. Hagemeier, “Introduction to the Opioid Epidemic: The Economic Burden on the Healthcare System and Quality of Life,” American Journal of Managed Care 24 (2018): S200-S206.
[21] Abby Alpert, David Powell, and Rosalie Liccardo Pacula, “Supply-Side Drug Policy in the Presence of Substitutes: Evidence from the Introduction of Abuse-Deterrent Opioids,” Economic Policy 10, no. 4 (2018): 1-35.
[22] Council of Economic Advisors, “The Role of Opioid Prices in the Evolving Opioid Epidemic,” Trump White House Archives, 2019.
[23] Hui Cheng, and Paul M. Copland, “Incidence of Nonmedical Use of OxyContin and Other Prescription Opioid Pain Relievers Before and After the Introduction of OxyContin with Abuse Deterrent Properties,” Postgraduate Medicine 130, no. 6 (2018): 568-574; Catherine S. Hwang, Hsien-Yen Chang, and G. Caleb Alexander, “Impact of Abuse-Deterrent OxyContin on Prescription Opioid Utilization,” Pharmacoepidemiol Drug Safety 24, no. 2 (2015): 197-204; Marc R. Larochelle, Fang Zhang, Dennis Ross-Degnan, and J. Frank Wharam, “Rates of Opioid Dispensing and Overdose After Introduction of Abuse-Deterrent Extended-Release Oxycodone and Withdrawal of Propoxyphene,” JAMA Internal Medicine 175, no. 6 (2015): 978-987.
[24] Centers for Disease Control and Prevention, “Understanding the Epidemic,” U.S. Department of Health and Human Services, 2021.
[25] Abby Alpert, David Powell, and Rosalie Liccardo Pacula, “Supply-Side Drug Policy in the Presence of Substitutes: Evidence from the Introduction of Abuse-Deterrent Opioids,” Economic Policy 10, no. 4 (2018): 1-35; William N. Evans, Ethan M.J. Lieber, and Patrick Power, “How the Reformulation of OxyContin Ignited the Heroin Epidemic,” The Review of Economics and Statistics 101, no. 1 (2019): 1-15; Jeffrey Singer, “Abuse-Deterrent Opioids and the Law of Unintended Consequences,” Cato Institute, February 6, 2018; Carolyn Wolff, William N. Dowd, Mir M. Ali, Chandler McClellan, Angelica Meinhofer, Lukas Glos, Ryan Mutter, Matthew Rosenberg, and Andreas Schick, “The Impact of the Abuse-Deterrent Reformulation of OxyContin on Prescription Pain Reliever Misuse and Heroin Initiation,” Addictive Behaviors 105 (2020).
[26] Sandra D. Comer, Maria A. Sullivan, Robert A. Whittington, Suzanne K. Vosburg, and William J. Kowalcyzk, “Abuse Liability of Prescription Opioids Compared to Heroin in Morphine-Maintained Heroin Abusers,” Neuropsychopharmacology 33, no. 5 (2008): 1179-1191.
[27] National Institute on Drug Abuse, “A Subset of People Who Abuse Prescription Opioids May Progress to Heroin Use,” March 17, 2021.
[28] Theodore J Cicero, Matthew S. Ellis, Hilary L. Surratt, and Steven P. Kurtz. “The Changing Face of Heroin Use in the United States: A Retrospective Analysis of the Past 50 Years,” JAMA Psychiatry 71, no. 7 (2014): 821.
[29] Daniel Ciccarone, “The Triple Wave Epidemic: Opioids, Heroin, and Fentanyl” (lecture, the University of California-San Francisco, San Francisco, CA, August 19, 2019).
[30] Claire Felter, “The U.S. Opioid Epidemic,” Council on Foreign Relations, September 8, 2021
[31] National Institute on Drug Abuse, “Why Does Heroin Use Create Special Risk for Contracting HIV/AIDS and Hepatitis B and C?,” April 13, 2021. These indirect deaths are not factored into opioid overdose death sums as calculated by the Centers for Disease Control and Prevention.
[32] Emily Feng, “‘We Are Shipping to the U.S.:’ Inside China’s Online Synthetic Drug Networks,” NPR, November 17, 2020; Liana W. Rosen and Susan V. Lawrence, “Illicit Fentanyl and China’s Role,” Congressional Research Service, January 29, 2021; Drug Enforcement Administration, “Dealer Admits Selling Deadly Fentanyl Laced Pills,” U.S. Department of Justice, September 16, 2019; U.S. House of Representatives, Committee on Energy and Commerce, Fentanyl: The Next Wave of the Opioid Crisis, 115th Cong., 1st sess., March 21, 2017.
[33] Minnesota Department of Health, “Fentanyl Analogs,” 2020.
[34] Drug Enforcement Administration, “DEA Issues Carfentanil Warning to Police and Public,” U.S. Department of Justice, September 22, 2016.
[35] Drug Enforcement Administration, “National Drug Threat Assessment,” U.S. Department of Justice, 2017.
[36] Lisa N. Sacco, Kristin Finklea, Susan V. Lawrence, Liana W. Rosen, Clare Ribando Seelke, “The Opioid Epidemic: Supply Control and Criminal Justice Policy — Frequently Asked Questions,” Congressional Research Service, June 28, 2019; Kristin Finklea, “Heroin Trafficking in the United States,” Congressional Research Service, February 14, 2019.
[37] Drug Enforcement Administration, “Fentanyl Flow to the United States,” U.S. Department of Justice, March 6, 2020.
[38] Ibid.
[39] Liana W. Rosen and Susan V. Lawrence, “Illicit Fentanyl and China’s Role,” Congressional Research Service, January 29, 2021.
[40] Drug Enforcement Administration, “Fentanyl,” U.S. Department of Justice, 2021; Los Angeles County Department of Public Health, “Fentanyl,” 2020; United States Sentencing Commission, “Fentanyl and Fentanyl Analogs,” United States Sentencing Commission, January 25, 2021.
[41] Minnesota Department of Health, “Fentanyl Analogs,.” 2020.
[42] U.S. House of Representatives, Committee on Energy and Commerce, Fentanyl: The Next Wave of the Opioid Crisis, 115th Cong., 1st sess., March 21, 2017.
[43] Centers for Disease Control and Prevention, “Understanding the Epidemic,” U.S. Department of Health and Human Services, 2021.
[44] Ibid.
[45] This paper does not actively investigate fentanyl since it is not opioid-based, as research by Deiana et al. found no link between Afghan opium and fentanyl use.
[46] Jonathan H. Duff, “Opioid Treatment Programs and Related Federal Regulations,” Congressional Research Service, June 12, 2019; Anne Schuchat, Debra Houry, and Gery P. Guy Jr., “New Data on Opioid Use and Prescribing in the United States,” Journal of the American Medical Association 318, no. 5 (2017): 425-426.
[47] David J. Goodman, “Naloxone, a Drug to Stop Heroin Deaths, is More Costly, the Police Say,” The New York Times, December 1, 2014.
[48] Lisa N. Sacco, Kristin Finklea, Susan V. Lawrence, Liana W. Rosen, and Clare Ribando Seelke, “The Opioid Epidemic: Supply Control and Criminal Justice Policy — Frequently Asked Questions,” Congressional Research Service, June 28, 2019.
[49] Sarah Braner, “An Epidemic in the Shadow of a Pandemic: Drug Overdose Deaths Reach an All-Time High in the U.S.,” CNN, July 17, 2021.
[50] Gretchen Peters, “How Opium Profits the Taliban,” United States Institute of Peace, August 2, 2009; Office of National Drug Control Policy, “The International Heroin Market,” Obama White House Archives, 2010; United Nations Office on Drugs and Crime, “Afghan Opium Survey 2019,” The United Nations, 2020.
[51] United Nations Office on Drugs and Crime, “Addiction, Crime, and Insurgency: The Transnational Threat of Afghan Opium,” The United Nations, 2009.
[52] Ali Wardak, “Integrated Social Control in Afghanistan: Implications for the Licensed Cultivation of Poppy for the Production of Medicines,” The International Council on Security and Development (2006).
[53] John Miltenburg, “Supply Chains for Illicit Products: Case Study of the Global Opiate Production Networks,” Cogent Business & Management 5, no. 1 (2018).
[54] Office of National Drug Control Policy, “The International Heroin Market,” Obama White House Archives, 2010.
[55] David Mansfield and Adam Pain, “Alternative Livelihoods: Substance or Slogan?,” Afghan Research and Evaluation Unit, October 1, 2005; Center for Advanced Defense Studies, “Opium in Afghanistan: Lawlessness Thrives on Narcotics Trade,” June 2006.
[56] Justin Rowlatt, “What the Heroin Industry Can Teach Us About Solar Power,” BBC News, July 27, 2020.
[57] Victoria A. Greenfield, Keith Crane, Craig A. Bond, Nathan Chandler, Jill E. Luoto, and Olga Oliker. “Reducing the Cultivation of Opium Poppies in Southern Afghanistan,” RAND Corporation, 2015; David Mansfield and Adam Pain, “Alternative Livelihoods: Substance or Slogan?,” Afghan Research and Evaluation Unit, October 1, 2005.
[58] Azan Ahmed, “Tasked with Combating Opium, Afghan Officials Profit from It,” The New York Times, February 16, 2016; Gretchen Peters, “How Opium Profits the Taliban,” United States Institute of Peace, August 2, 2009; Armando Geller, Seyed M. Mussavi Rizi, and Maciej M. Łatek. “How Corruption Blunts Counternarcotic Policies in Afghanistan: A Multiagent Investigation.” Social Computing, Behavioral-Cultural Modeling, and Prediction 4 (2011): 121-128.
[59] Graham Farrell and John Thorne, “Where Have All the Flowers Gone?: Evaluation of the Taliban Crackdown Against Opium Poppy Cultivation in Afghanistan,” International Journal of Drug Policy 16, no. 2 (2005): 81-91.
[60] United Nations Office on Drugs and Crime, “Addiction, Crime, and Insurgency: The Transnational Threat of Afghan Opium,” The United Nations, 2009.
[61] Jonathan Goodhand, “From Holy War to Opium War? A Case Study of the Opium Economy in North Eastern Afghanistan,” Disasters 24, no. 2 (2000): 87-102; United Nations Office on Drugs and Crime, The Opium Economy in Afghanistan: An International Problem. New York: UNODC, 2003; Jeffrey Bartholet, “The Holy Men of Heroin,” Newsweek, December 5, 1999.
[62] Matthew C. Dupee, “The Narcotics Emirate of Afghanistan: Examining Armed Policies and Their Roles in the Illicit Drug Production and Conflict in Afghanistan 1980-2010,” Master’s thesis (Naval Postgraduate School, 2010).
[63] Gretchen Peters, “How Opium Profits the Taliban,” United States Institute of Peace, August 2, 2009; William A. Byrd and Olivier Jonglez, “Prices and Market Interactions in the Opium Economy,” World Bank / The United Nations, 2006.
[64] Graham Farrell and John Thorne, “Where Have All the Flowers Gone?: Evaluation of the Taliban Crackdown Against Opium Poppy Cultivation in Afghanistan,” International Journal of Drug Policy 16, no. 2 (2005): 81-91.
[65] David Mansfield and Adam Pain, “Alternative Livelihoods: Substance or Slogan?,” Afghan Research and Evaluation Unit, October 1, 2005.
[66] United Nations Office on Drugs and Crime, “Afghan Farmers’ Intentions Survey 2003/2004,” The United Nations, 2004.
[67] United Nations Office on Drugs and Crime, “Afghan Farmers’ Intentions Survey 2003/2004,” The United Nations, 2004.
[68] Bureau of International Narcotics and Law Enforcement Affairs, “International Narcotics Control Strategy Report,” U.S. Department of State, March 2, 2021.
[69] Ibid.
[70] See Data for an in-depth description of the nomenclature of potential opium production.
[71] United Nations Office on Drugs and Crime, “World Drug Report 2010,” The United Nations, 2010.
[72] Jasmine Bhatia, “Drugs and (Dis)Order in Afghanistan,” Global Challenges Research Fund, April 2020.
[73] Justin Rowlatt, “How the US Military’s Opium War in Afghanistan was Lost,” BBC News, April 25, 2019.
[74] George Unick, Daniel Rosenblum, Sarah Mars, and Daniel Ciccarone, “The Relationship Between US Heroin Market Dynamics and Heroin-Related Overdose, 1992-2000,” Addiction 109, no. 11 (2014): 1889-1998.
[75] United Nations Office on Drugs and Crime, “World Drug Report 2010,” The United Nations, 2010.
[76] Vanda Felbab-Brown, “Afghanistan’s Opium Production is Through the Roof – Why Washington Shouldn’t Overreact,” Brookings Institution, November 21, 2017.
[77] David Mansfield and William Byrd, “Licensing Afghan Opium for Medical Use: Why it Won’t Work,” United States Institute of Peace, September 25, 2014.
[78] Sandra D. Comer, Maria A. Sullivan, Robert A. Whittington, Suzanne K. Vosburg, and William J. Kowalcyzk, “Abuse Liability of Prescription Opioids Compared to Heroin in Morphine-Maintained Heroin Abusers,” Neuropsychopharmacology 33, no. 5 (2008): 1179-1191.
[79] Sarah G. Mars, Daniel Rosenblum, and Daniel Ciccarone, “Illicit Fentanyls in the Opioid Street Market: Desired or Imposed?,” Addiction 114, no. 5 (2018): 774-780; Sarah Braner, “An Epidemic in the Shadow of a Pandemic: Drug Overdose Deaths Reach an All-Time High in the U.S.,” CNN, July 17, 2021; Drug Enforcement Administration, “Dealer Admits Selling Deadly Fentanyl Laced Pills,”U.S. Department of Justice, September 16, 2019.
[80] John E. DiNardo and Thomas Lemieux, “Alcohol, Marijuana, and American Youth: The Unintended Effects of Government Regulation,” Journal of Health Economics 20, no. 6 (2001): 991-1010; Benjamin Crost and Santiago Guerrero, “The Effect of Alcohol Availability on Marijuana Use: Evidence from the Minimum Legal Drinking Age,” Journal of Health Economics 31, no. 1 (2012): 112-121.
[81] Abby Alpert, David Powell, and Rosalie Liccardo Pacula, “Supply-Side Drug Policy in the Presence of Substitutes: Evidence from the Introduction of Abuse-Deterrent Opioids,” Economic Policy 10, no. 4 (2018): 1-35.
[82] William N. Evans, Ethan M.J. Lieber, and Patrick Power. “How the Reformulation of OxyContin Ignited the Heroin Epidemic.” The Review of Economics and Statistics 101, no. 1 (2019): 1-15.
[83] Sandra D. Comer, Maria A. Sullivan, Robert A. Whittington, Suzanne K. Vosburg, and William J. Kowalcyzk, “Abuse Liability of Prescription Opioids Compared to Heroin in Morphine-Maintained Heroin Abusers,” Neuropsychopharmacology 33, no. 5 (2008): 1179-1191.
[84] National Institute on Drug Abuse, “Heroin Use is Driven by its Low Cost and High Availability,” April 13, 2021.
[85] Jeffrey Singer, “The Abuse-Deterrent Folly,” Cato Institute, September 12, 2020.
[86] Claudio Deiana, Ludovica Giua, and Roberto Nisticó, “The Economics Behind the Epidemic: Afghan Opium Price and Prescription Opioids in the U.S.,” IZA Institute of Labor Economics, Discussion Paper Series No. 12872, 2019.
[87] United Nations Office on Drugs and Crime, The Opium Economy in Afghanistan: An International Problem, New York: UNODC, 2003; United Nations Office on Drugs and Crime, “The Global Afghan Opium Trade: A Threat Assessment,” The United Nations, July 20, 2011.
[88] National Institute on Drug Abuse, “A Subset of People Who Abuse Prescription Opioids May Progress to Heroin Use,” March 17, 2021.
[89] Rosanna Smart, Bryce Pardo, and Corey S. Davis, “Systematic Review of the Emerging Literature on the Effectiveness of Naloxone Access Laws in the United States,” Addiction 116, no. 1 (2021): 16-17.
[90] Jan C. van Ours, “The Price Elasticity of Hard Drugs: The Case of Opium in the Dutch East Indies, 1923-1938,” Journal of Political Economy 103, no. 2 (1995): 261-279.
[91] Jin-Long Liu, Jin-Tan Liu, James K. Hammitt, and Shin-Yi Chou. “The Price Elasticity of Opium in Taiwan, 1914-1942.” Journal of Health Economics 18, no. 6 (1999): 795-810.
[92] Lester P. Silverman and Nancy L. Spruill, “Urban Crime and the Price of Heroin,” Journal of Urban Economics 4, no. 1 (1977): 80-103.
[93] Jonathan P. Caulkins, “Estimating Elasticities of Demand for Cocaine and Heroin with Data from the Drug Use Forecasting System,” United States Department of Justice, 1995.
[94] Henry Saffer and Frank Chaloupka, “The Demand for Illicit Drugs,” Economic Inquiry 37 (2007): 401-411.
[95] Nancy Petry and Warren K. Bickel, “Polydrug Abuse in Heroin Addicts: A Behavioral Economic Analysis,” Addiction 93, no. 3 (1998): 321-325.
[96] Mireia Jofre-Bonet and Nancy Petry, “Trading Apples for Oranges?: Results of an Experiment on the Effects of Heroin and Cocaine Price Changes on Addicts’ Polydrug Use,” Journal of Economic Behavior & Organization 66, no. 2 (2008): 281-311.
[97] Jerry Chalmers, Deborah Bradford, and Craig Jones, “The Effect of Methamphetamine and Heroin Price on Polydrug Use: A Behavioural Economics Analysis in Sydney, Australia,” International Journal of Drug Policy 21, no. 5 (2010): 381-389.
[98] Dhaval Dave, “Illicit Drug Use Among Arrestees, Prices and Policy,” Journal of Urban Economics 63, no. 2 (2008): 694-714.
[99] Anne Linne Bretteville-Jensen and Erik Biørn, “Heroin Consumption, Prices and Addiction: -Evidence from Self-Reported Panel Data,” The Scandinavian Journal of Economics 105, no. 4 (2003): 661-679.
[100] Juliette Roddy and Mark Greenwald, “An Economic Analysis of Income and Expenditures by Heroin-Using Research Volunteers,” Substance Use & Misuse 44, no. 11 (2009): 1502-1518.
[101] Anne Linne Bretteville-Jensen, “Drug Demand – Initiation, Continuation and Quitting,” De Economist 154, no. 4 (2006): 491-516.
[102] Todd A. Olmstead, Sheila M. Alessi, Brendan Kline, Rosalie Liccardo Pacula, and Nancy M. Petry. “The Price Elasticity of Demand for Heroin: Matched Longitudinal and Experimental Evidence,” Journal of Health Economics 41 (2015): 59-71.
[103] Council of Economic Advisors, “The Role of Opioid Prices in the Evolving Opioid Epidemic,” Trump White House Archives, 2019.
[104] Justin Gatwood, Teresa B. Gibson, Michael E. Chernew, Amanda M. Farr, Emily Vogtmann, and A. Mark Fendrick. “Price Elasticity and Medication use: Cost Sharing Across Multiple Clinical Conditions,” Journal of Managed Care and Specialty Pharmacy 20, no. 11 (2014): 1102-1107.
[105] David Powell, Rosalio Liccardo Pacula, and Erin Taylor, “How Increasing Medical Access to Opioids Contributes to the Opioid Epidemic: Evidence from Medicare Part D,” Journal of Health Economics 71(2020): 102286.
[106] Justin C. Strickland, Joshua A. Lile, and William W. Stoops, “Evaluating Non-Medical Prescription Opioid Demand Using Commodity Purchase Tasks: Test-Retest Reliability and Incremental Validity,” Psychopharmacology 236 (2019): 2641-2652.
[107] Sarah G. Mars, Daniel Rosenblum, and Daniel Ciccarone, “Illicit Fentanyls in the Opioid Street Market: Desired or Imposed?,” Addiction 114, no. 5 (2018): 774-780.
[108] National Institute on Drug Abuse, “A Subset of People Who Abuse Prescription Opioids May Progress to Heroin Use,” March 17, 2021; Gary S. Becker, Michael Grossman, and Kevin M. Murphy, “Rational Addiction and the Effect of Price on Consumption,” The American Economic Review 81, no. 2 (1991): 237-241.
[109] George Unick, Daniel Rosenblum, Sarah Mars, and Daniel Ciccarone, “The Relationship Between US Heroin Market Dynamics and Heroin-Related Overdose, 1992-2000,” Addiction 109, no. 11 (2014): 1889-1998.
[110] Claudio Deiana, Ludovica Giua, and Roberto Nisticó, “The Economics Behind the Epidemic: Afghan Opium Price and Prescription Opioids in the U.S.,” IZA Institute of Labor Economics, Discussion Paper Series No. 12872, 2019.
[111] Ibid.
[112] Ibid.
[113] Christopher Blanchard, “Afghanistan: Narcotics and U.S. Policy,” Congressional Research Service, August 12, 2009; United Nations Office on Drugs and Crime, “Addiction, Crime, and Insurgency: The Transnational Threat of Afghan Opium,” The United Nations, 2009.
[114] Joseph G. Millan, “Poppy Cultivation in Afghanistan: A Global Strategic Nemesis,” Master’s thesis, (United States Army War College, April 7, 2003).
[115] United Nations Office on Drugs and Crime, “Afghan Farmers’ Intentions Survey 2003/2004,” The United Nations, 2004.
[116] United Nations Office on Drugs and Crime, “Addiction, Crime, and Insurgency: The Transnational Threat of Afghan Opium,” The United Nations, 2009.
[117] John Miltenburg, “Supply Chains for Illicit Products: Case Study of the Global Opiate Production Networks,” Cogent Business & Management 5, no. 1 (2018); United Nations Office on Drugs and Crime, The Opium Economy in Afghanistan: An International Problem, New York: UNODC, 2003.
[118] Martha B. Olcott and Natalia Udalova Zwart. “Drug Trafficking on the Great Silk Road: The Security Environment in Central Asia.” Carnegie Endowment for International Peace, March 1, 2000.
[119] Miguel Marchildon, “An Application of the Gravity Model to International Trade in Narcotics.” Master’s thesis (University of Ottawa, 2018).
[120] James E. Anderson, “The Gravity Model,” National Bureau of Economic Research (Working Paper 16576), December 2010.
[121] Alex Stevens, Drugs, Crime and Public Health: The Political Economy of Drug Policy, New York: Routledge, 2011; William Walker, Opium and Foreign Policy: The Anglo-American Search for Order in Asia, 1912-1954, Chapel Hill: University of North Carolina Press, 1991; Brandon J. Swartz, “Afghanistan Connection: Heroin Production, Distribution, and Consumption,” Master’s thesis (Michigan Technological University, 2011).
[122] Daniel Rosenblum, George J. Unick, and Daniel Ciccarone, “The Entry of Colombian-Sourced Heroin into the US Market: The Relationship Between Competition, Price, and Purity,” International Journal of Drug Policy 25, no. 1 (2014): 88-95.
[123] David Mansfield and Adam Pain, “Alternative Livelihoods: Substance or Slogan?,” Afghan Research and Evaluation Unit, October 1, 2005; Claudio Deiana, Ludovica Giua, and Roberto Nisticó, “The Economics Behind the Epidemic: Afghan Opium Price and Prescription Opioids in the U.S.,” IZA Institute of Labor Economics, Discussion Paper Series No. 12872, 2019.
[124] United Nations Office on Drugs and Crime, “The Global Afghan Opium Trade: A Threat Assessment,” The United Nations, July 20, 2011.
[125] United Nations Office on Drugs and Crime, “Afghan Opiate Trafficking Along the Northern Route,” The United Nations, June 16, 2018.
[126] Jeffrey Fudin, “Individual Patient and Medication Factors that Invalidate Morphine Milligram Equivalents,” lecture at FDA collaborative, June 8, 2021.
[127] Casey Mulligan, “Prices and Federal Policies in Opioid Markets.” National Bureau of Economic Research (Working Paper 26812), February 2020.
[128] FDA price calculations, weighted in a way that reflects changes in prescription opioid prices during the epidemic’s transition towards illicit opioids, were provided by Dr. Casey Mulligan of the University of Chicago via email.
[129] Data describing heroin retail prices, collected by the DEA and organized by the UNODC, were adjusted for fentanyl content as per the methods of the Council of Economic Advisors (2019), and also provided by Dr. Mulligan, who wrote in 2020 that “Heroin prices are from [the] United Nations Office on Drugs and Crime (2018) and the various Drug Threat Assessments published by the U.S. Drug Enforcement Administration, as well as supplementary estimates made by Council of Economic Advisers.”
[130] Substance Abuse and Mental Health Services Administration, “Using International Classification of Diseases (ICD) Codes to Assess Opioid-Related Overdose Deaths,” U.S. Department of Health and Human Services (2021).
[131] Ibid.
[132] Alfred W. McCoy, “From Free Trade to Prohibition: A Critical History of the Modern Asian Opium Trade,” Fordham Urban Law Journal 28, no. 1 (2000): 307-349.
[133] United Nations Office on Drugs and Crime, “World Drug Report 2008: Methodology,” The United Nations, 2008.
[134] Uppsala Conflict Data Program, “Afghanistan.”
[135] World Bank, “World Development Indicators,” 2019.
[136] Ibid.
[137] United Nations Department of Economic and Social Affairs, “Annual Total Population at Mid-Year (Thousands),” The United Nations, 2021.
[138] Mary C. Acock, Zhongchun Wang, and Basil Acock, “Phases of Development to Flowering in Opium Poppy (Papaver somniferum L.) under Various Temperatures,” Annals of Botany 80, no. 4 (1997): 547-552.
[139] Edwin Snyder, “War, Drugs, and Money: The Opium Trade in Afghanistan,” Master’s thesis (Harvard University, 2019).
[140] Alex Hollingsworth, Christopher J. Ruhm, and Kosali Simon, “Macroeconomic Conditions and Opioid Abuse,” Journal of Health Economics 56 (2017): 222-233.
[141] Paul Contoyannis, Jeremiah Hurley, Paul Grootendorst, Sung-Hee Jeon, and Robyn Tamblyn, “Estimating the Price Elasticity of Expenditure for Prescription Drugs in the Presence of Non-Linear Price Schedules: An Illustration from Quebec, Canada,” Health Economics 14, no. 6 (2005): 909-923.
[142] Federal Reserve Bank of St. Louis, “Unemployment Rate,” 2021.
[143] Substance Abuse and Mental Health Services Administration, “Using International Classification of Diseases (ICD) Codes to Assess Opioid-Related Overdose Deaths,” U.S. Department of Health and Human Services (2021).
[144] Alex Hollingsworth, Christopher J. Ruhm, and Kosali Simon, “Macroeconomic Conditions and Opioid Abuse,” Journal of Health Economics 56 (2017): 222-233.
[145] United Nations Office on Drugs and Crime, “Afghan Farmers’ Intentions Survey 2003/2004,” The United Nations, 2004; United Nations Office on Drugs and Crime, “Summary Findings of Opium Trends in Afghanistan, 2005,” The United Nations, September 6, 2005.
[146] Gretchen Peters, “How Opium Profits the Taliban,” United States Institute of Peace, August 2, 2009.
[147] Azan Ahmed, “Tasked with Combating Opium, Afghan Officials Profit from It,” The New York Times, February 16, 2016.
[148] David J. Liddell, “Drugs in Afghanistan: The Challenges With Implementing U.S. Strategy,” Master’s thesis (United States Army War College, March 15, 2008).
[149] These figures were calculated by multiplying coefficients from the first- and second-stage results, and are graphed in Figure 9 below.
[150] Justin Rowlatt, “What the Heroin Industry Can Teach Us About Solar Power,” BBC News, July 27, 2020.
[151] Note that a potential endogeneity problem exists, in that less opium may be attempted to be cultivated by farmers in the first place as the weather in a given year appears less favorable.
[152] Mary C. Acock, Zhongchun Wang, and Basil Acock, “Phases of Development to Flowering in Opium Poppy (Papaver somniferum L.) under Various Temperatures,” Annals of Botany 80, no. 4 (1997): 547-552.
[153] Ahmet Gümüşçü and Gönül Gümüşçü, “Climate Change and Effect on Yield Components of Opium Poppy,” Turkish Economic Review 24, no. 1 (2015): 79-84.
[154] World Bank, “Climate Change Knowledge Portal,” 2020.
[155] Resul Cesur, Joseph J. Sabia, and W. David Bradford. “Did the War on Terror Ignite an Opioid Epidemic?” National Bureau of Economic Research (Working Paper 26264), September 2019; Onur Basur, Lin Xie, Jack Mardekian, David Schaaf, Li Wang, and Ashish V. Joshi, “Prevalence of Diagnosed Opioid Abuse and its Economic Burden in the Veterans Health Administration,” Pain Practice 14, no. 5 (2013): 437-445.
[156] Centers for Disease Control and Prevention, “Understanding the Epidemic,” U.S. Department of Health and Human Services, 2021.
[157] John Miltenburg, “Supply Chains for Illicit Products: Case Study of the Global Opiate Production Networks,” Cogent Business & Management 5, no. 1 (2018); Drug Enforcement Administration, “Synthetic Opioids,” U.S. Department of Justice, 2020.
[158] Jacob N. Miller, “The War on Drugs 2.0: Darknet Fentanyl’s Rise and the Effects of Regulatory and Law Enforcement Action,” Contemporary Economic Policy 38, no. 2 (2019): 246-257.
[159] Claudio Deiana, Ludovica Giua, and Roberto Nisticó, “The Economics Behind the Epidemic: Afghan Opium Price and Prescription Opioids in the U.S.,” IZA Institute of Labor Economics, Discussion Paper Series No. 12872, 2019.
[160] Francois Lamy, Raminta Daniulaityte, Monica J. Barrett, Usha Lokala, Amit Sheth, and Robert G. Carlson, “Listed for Sale: Analyzing Data on Fentanyl, Fentanyl Analogs and Other Novel Synthetic Opioids on One Cryptomarket,” Drug and Alcohol Dependence 213, no. 1 (2010): 108-115.
[161] Jacob N. Miller, “The War on Drugs 2.0: Darknet Fentanyl’s Rise and the Effects of Regulatory and Law Enforcement Action,” Contemporary Economic Policy 38, no. 2 (2019): 246-257.
[162] Roderic Broadhurst, Matthew Ball, and Harshit Trivedi, “Fentanyl Availability on Darknet Markets,” Trends and Issues in Crime and Criminal Justice (2020): 790.
[163] Nabarun Dasgupta, Clark Freifeld, John S. Brownstein, Christopher Mark Menone, Hilary L. Surratt, Luke Poppish, Jody L. Green, Eric J. Lavonas, and Richard C. Dart, “Crowdsourcing Black Market Prices for Prescription Opioids,” Journal of Medical Internet Research 15, no. 8 (2013): e178.
[164] Johanna Catherine Maclean, Justine Mallatt, Christopher J. Ruhm, and Kosali Simon, “Economic Studies on the Opioid Crisis: A Review,” National Bureau of Economic Research (Working Paper 28067), 2020; Daniel Werb, Thomas Kerr, Julio Montaner, and Evan Wood, “The Need for an Evidence-Based Approach to Controlling Opium Production in Afghanistan,” Journal of Public Health Policy 29, no. 4 (2008): 440-448.
[165] Joel Hafvenstein, Opium Season: A Year on the Afghan Frontier. Guilford: Lyons Press, 2009.
[166] David J. Liddell, “Drugs in Afghanistan: The Challenges With Implementing U.S. Strategy,” Master’s thesis (United States Army War College, March 15, 2008).
[167] Frederic Grare, “Anatomy of a Fallacy: The Senlis Council and Narcotics in Afghanistan,” Carnegie Endowment for International Peace, February 27, 2008; David Mansfield and William Byrd, “Licensing Afghan Opium for Medical Use: Why it Won’t Work,” United States Institute of Peace, September 25, 2014; David Mansfield and Adam Pain, “Opium Poppy Eradication: How to Raise Risk When There is Nothing to Lose?,” Afghan Research and Evaluation Unit, August 1, 2006.
[168] Council of Economic Advisors, “The Role of Opioid Prices in the Evolving Opioid Epidemic,” Trump White House Archives, 2019.